When and How to Start Tapering: Methods, Symptoms, and What Fits You
⚕️ This article is education, not medical advice. Every claim is sourced below. Never stop or change medication without your prescriber — some medications are dangerous to stop abruptly.
TL;DR: There is no universal “right time” to start tapering — the useful test is whether you are reasonably stable, not in the middle of a crisis, and working with a prescriber who agrees the benefits of reducing outweigh the risks for you. Once you start, the method matters: guidelines increasingly favour gradual proportional (hyperbolic) reductions over fixed-size cuts, with the pace set by how your body responds rather than a calendar. Expect symptoms to come and go, use holding and reinstatement as normal course-corrections, and match the approach to your drug class and history. This article is education, not medical advice; some medications — benzodiazepines especially — are dangerous to stop quickly, so plan every change with your prescriber.
When is the right time to start tapering?
The honest answer is that timing is a judgment, not a formula. Deprescribing guidelines frame it as a shared decision between you and your prescriber, weighing how long you’ve taken the drug, why you started, how you’re doing now, and what you want. A few conditions make tapering more likely to go well:
- You’re relatively stable. Reducing a medication is easier when your underlying condition is settled and you have some capacity to cope with fluctuations.
- You’re not in the middle of a crisis. Major life stress — a bereavement, a job loss, a move — is usually a reason to wait, not to start.
- The reason to reduce is clear. Side effects, a resolved original problem, a wish to stop, or a drug that guidelines flag for long-term risk (like benzodiazepines) are all legitimate reasons.
- You have support and a plan. A prescriber who will follow up, and a way to track how it’s going, both matter more than the exact month you begin.
Equally, there are times to hold off: acute illness, unstable symptoms, or no realistic support for follow-up. Starting slowly and being willing to pause is safer than forcing a schedule. If you’re unsure how to raise it, our guide on talking to your doctor about deprescribing can help.
Why can’t I just stop, or cut the dose in half?
Because the body adapts to a medication’s presence, and undoing that adaptation takes time. Two facts drive this:
- Withdrawal is common and often underestimated. A 2019 systematic review by Davies and Read found that among people who stopped antidepressants, a large proportion experienced withdrawal symptoms, a meaningful share rating them as severe. Stopping abruptly maximizes this.
- Dose and effect are not a straight line. For many drugs, receptor occupancy follows a hyperbolic curve — at higher doses, big milligram cuts change the biological effect only a little, but at low doses, the same milligram cut removes a large share of the remaining effect. This is why the last few milligrams are often the hardest, and why fixed-size steps get progressively harsher (see receptor occupancy explained).
Together these explain the modern preference for slow, proportional reductions over a “halve it, then stop” approach.
What are the main tapering methods?
There isn’t one method — there’s a toolkit, and different tools suit different drugs and doses.
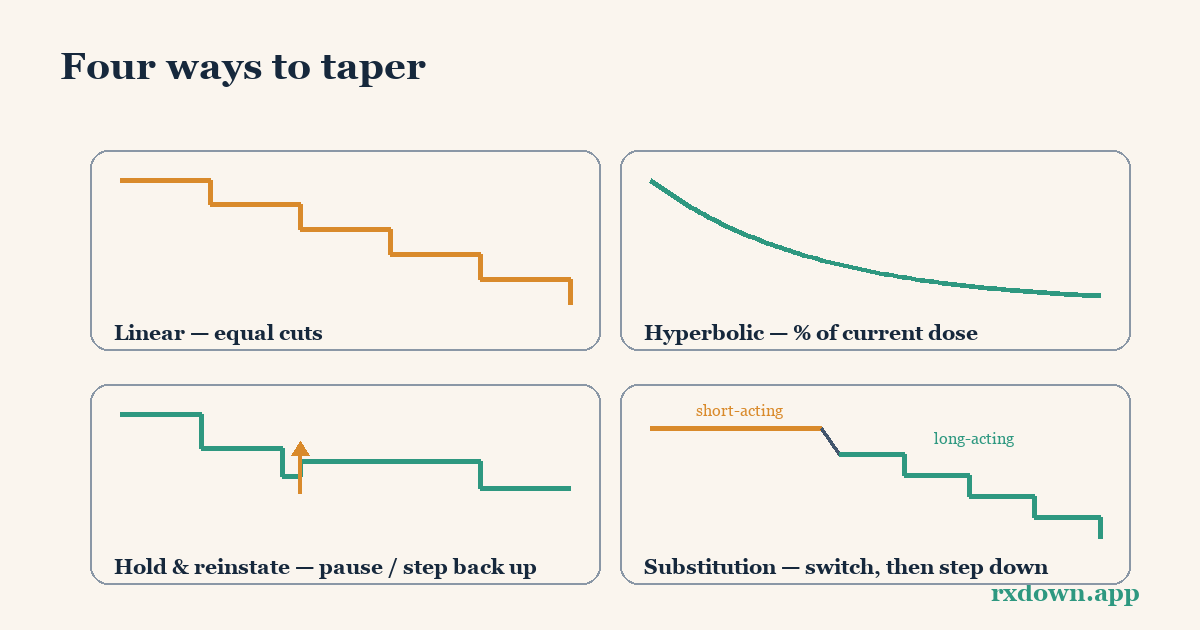
- Linear taper — equal-sized cuts (e.g., the same number of milligrams each step). Simple, but because of the hyperbolic curve it tends to feel easy at first and harsh near the end.
- Hyperbolic / proportional taper — each cut is a percentage of the current dose (often around 10%, individualized), so the absolute reductions shrink as the dose falls. This aims to produce a roughly even biological change at each step and is the approach the Maudsley Deprescribing Guidelines and NICE describe for antidepressants.
- Tapering strips and compounded/liquid doses — practical ways to make the very small doses that hyperbolic tapering needs but standard tablets can’t provide. Groot and van Os’s cohort work showed tapering strips help people achieve these fine reductions.
- Substitution (the Ashton approach for benzodiazepines) — switching a short-acting benzodiazepine to a long-acting one (typically diazepam) before stepping down, to smooth out the peaks and troughs. Detailed in the Ashton Manual guide.
- Holding and reinstatement — pausing at a dose until symptoms settle, or briefly stepping back up if they flare. These are standard course-corrections, not signs of failure (see hold and reinstate).
| Method | How it works | Best suited to | Caveats |
|---|---|---|---|
| Linear | Equal mg cuts each step | Short courses, higher-dose ranges | Gets harder near the end |
| Hyperbolic / proportional | % of current dose each step | Antidepressants, long-term use | Needs small doses (liquids/strips) |
| Tapering strips / liquids | Enables tiny, precise reductions | Anyone doing the low-dose end | Availability varies by country |
| Substitution (Ashton) | Switch to long-acting, then reduce | Short-acting benzodiazepines | Prescriber-guided; benzo-specific |
| Hold / reinstate | Pause or briefly step back up | Symptom flares at any stage | A plan, not a self-rescue for big doses |
What symptoms should I expect, and what do they tell me?
Withdrawal symptoms vary by drug class, but some patterns are common: rebound insomnia and anxiety, dizziness, flu-like feelings, “brain zaps” with antidepressants, irritability, and mood swings. Two things are worth understanding:
- Recovery is rarely linear. Many people describe alternating “windows and waves” — good stretches broken by returns of symptoms — rather than a steady climb.
- Symptoms are your pacing signal. Withdrawal effects that don’t settle before the next planned cut mean the pace is too fast. This is where holding or a small reinstatement is the right move. Distinguishing withdrawal from a genuine return of the original condition (relapse) matters too, because they call for different responses — our guide on withdrawal vs. relapse covers the tells.
Because symptoms guide the pace, tracking them against your dose over time is one of the most useful things you can do — memory alone bends toward however you feel today.
Which approach fits me?
The right plan depends on several factors you and your prescriber can weigh together:
- Drug class. Benzodiazepines and Z-drugs (GABA drugs) need cautious, often substitution-assisted tapers and must never be stopped abruptly from regular use. Antidepressants suit hyperbolic reductions. DORAs and melatonin agonists weren’t linked to withdrawal, so the issue there is mainly whether the original sleep problem returns. Not sure which you’re on? See know your medication.
- How long and how much. Longer use and higher doses generally call for slower tapers.
- Your history. If a previous attempt failed with harsh symptoms, that’s information — it usually points to a gentler, more gradual plan, not “try harder.”
- Your life right now. A stable period with support allows a steadier taper; a turbulent one argues for waiting or going slower.
- Your preferences. Some people want to move steadily; others prefer to hold longer at each step. Both can be valid.
The 2025 joint benzodiazepine tapering guideline and the Maudsley guidelines both stress individualization and flexibility over rigid schedules — the plan should adapt to you, not the other way round.
The bottom line
Start when you’re stable, supported, and your prescriber agrees — not on a fixed calendar. Favour gradual, proportional reductions over fixed-size cuts, use holds and small reinstatements as normal course-corrections, and let your symptoms set the pace. Match the method to your drug class and your history, and track dose against symptoms so the plan can adapt. Above all, some medications are dangerous to stop quickly, so make every change with your prescriber. To sketch a schedule to discuss, try the taper calculator; to understand the science behind proportional cuts, read hyperbolic tapering; and see the FAQ for more.
Sources
- Horowitz MA, Taylor D, Tapering of SSRI treatment to mitigate withdrawal symptoms, Lancet Psychiatry (2019)
- Horowitz M & Taylor D, The Maudsley Deprescribing Guidelines (Wiley-Blackwell, 2024)
- NICE, Depression in adults: treatment and management (NG222) (2022)
- NICE, Medicines associated with dependence or withdrawal symptoms (NG215) (2022)
- Ashton CH, Benzodiazepines: How They Work and How to Withdraw (The Ashton Manual, 2002/rev. 2011)
- Brunner E et al., Joint Clinical Practice Guideline on Benzodiazepine Tapering, Journal of General Internal Medicine (2025)
- Groot PC, van Os J, Successful use of tapering strips for hyperbolic reduction of antidepressant dose, Ther Adv Psychopharmacol (2021)
- Davies J, Read J, A systematic review into the incidence, severity and duration of antidepressant withdrawal effects, Addictive Behaviors (2019)
Frequently asked questions
When is a good time to start tapering a medication?
Generally when you are relatively stable, not in the middle of a crisis or major life stressor, and your prescriber agrees the potential benefits of reducing outweigh the risks. There is no universal timeline: guidelines emphasize a shared decision based on how long you've taken the drug, why you started, how you're doing now, and your own goals. Stability and a supported plan matter more than any fixed number of months, and some drugs should only be reduced very gradually.
What tapering method is best?
For most people on antidepressants, benzodiazepines, or Z-drugs, guidelines favour a gradual, proportional (hyperbolic) reduction — smaller and smaller absolute cuts as the dose falls — rather than fixed-size steps, because receptor effects are not linear. The 'best' method still depends on your drug, your dose, how you've responded to past changes, and how the reduction feels in practice. The right pace is the one your body tolerates, adjusted as you go with your prescriber.
How do I know if I'm tapering too fast?
Persistent or escalating withdrawal symptoms that don't settle before the next reduction are the main signal. In modern tapering, holding at the current dose until symptoms ease — or briefly reinstating a recent dose if they flare — is a normal course-correction, not a failure. Track symptoms against dose over time so you and your prescriber can see the trend and slow down if needed.
Tracking your dose, sleep, and symptoms makes every conversation in this article easier. RxDown is a free diary built for exactly that. Get RxDown · Free taper calculator