Windows and Waves: Why Withdrawal Recovery Isn't Linear
⚕️ This article is education, not medical advice. Every claim is sourced below. Never stop or change medication without your prescriber — some medications are dangerous to stop abruptly.
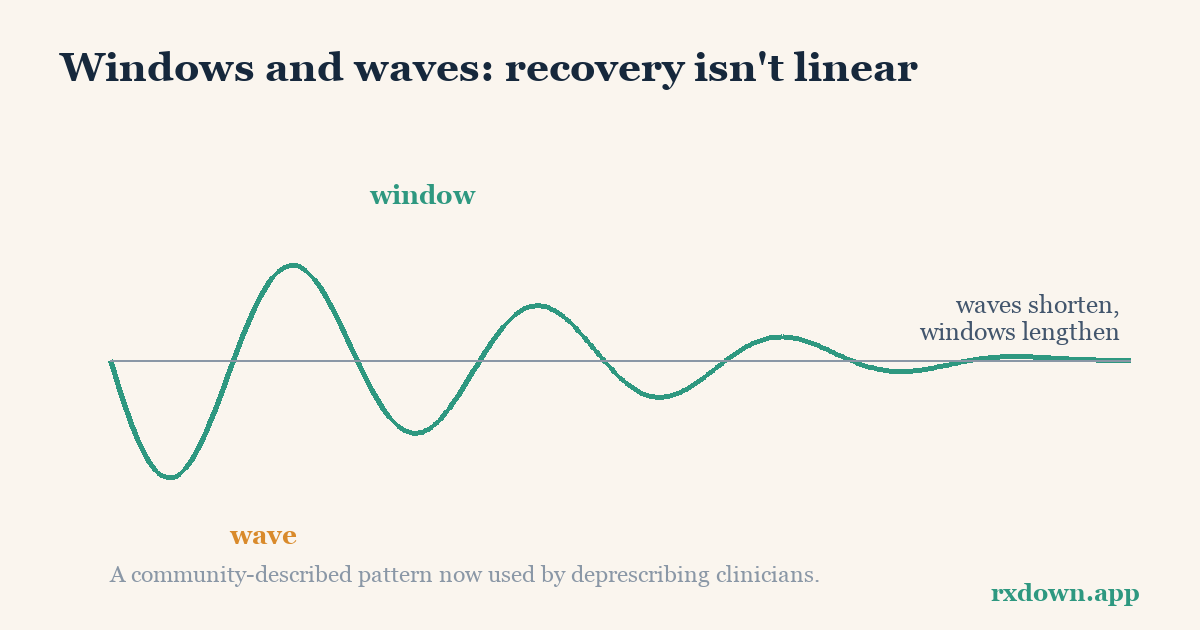
TL;DR: During and after medication withdrawal, many people notice a “windows and waves” pattern — stretches of feeling almost normal (windows) that alternate with the return of symptoms (waves). This up-and-down course is expected: the nervous system readapting to life without the drug is not a straight line, and stress, poor sleep, or illness can trigger a temporary wave. The single most useful thing to know is that a wave is not automatically relapse or permanent damage — over time windows usually get longer and waves usually get shorter. “Windows and waves” is a pattern first described by patient communities and now used by deprescribing clinicians; it is a helpful observational framework, not an RCT-validated diagnosis.
This article is education, not medical advice. Any change to a prescribed medication should be planned and supervised by your prescriber, and no medication should be stopped abruptly. If you are frightened by a wave, that reaction is normal — but it is a reason to talk with your clinician, not to make a rushed decision on your own.
What are “windows” and “waves” in withdrawal recovery?
A window is a period — it might last hours, days, or weeks — when withdrawal symptoms ease off or lift entirely and you feel close to your former self. A wave is the return or worsening of those symptoms that often follows a window. The two alternate, usually on no fixed schedule, and the shift between them can feel abrupt: someone can wake up in a wave after a week of feeling fine, with no obvious trigger.
The language comes from patient communities. Adele Framer, who founded the peer-support forum SurvivingAntidepressants.org and later co-authored clinical papers, describes how withdrawal symptoms “tend to surge irregularly as ‘waves and windows’” and how they “fluctuated and mutated” over the course of recovery (Framer, Therapeutic Advances in Psychopharmacology, 2021). The same vocabulary appears throughout benzodiazepine-tapering communities. It is worth being precise about evidence here: this is a pattern documented from thousands of patient reports and clinical experience, not a construct tested in randomized controlled trials. That does not make it unreal — it makes it observational, and worth tracking rather than assuming.
| Term | What it feels like | What it does not mean |
|---|---|---|
| Window | Symptoms fade; mood, sleep, and energy feel closer to baseline | It doesn’t mean you are “cured” and can skip the rest of the plan |
| Wave | Symptoms return or intensify, sometimes suddenly | It doesn’t automatically mean relapse or permanent harm |
Why isn’t withdrawal recovery a straight line?
Most people expect recovery to look like a smooth downhill slope: a bit better each week until you are back to normal. Withdrawal rarely behaves that way, and there are good physiological reasons.
Long-term use of a psychiatric or sleep medication produces neuroadaptation — the brain adjusts its receptor sensitivity and signaling to accommodate the drug’s constant presence. When the drug is reduced or removed, those adaptations have to unwind. That reversal is gradual and uneven, not instantaneous, which is why symptoms can persist and fluctuate after the last dose rather than switching cleanly off. Horowitz and Taylor’s work on how the brain responds to serotonin-targeting drugs is the basis for hyperbolic tapering — the finding that receptor occupancy changes steeply at low doses, so equal milligram cuts are not equal biological cuts (Horowitz & Taylor, The Lancet Psychiatry, 2019). The same non-linear pharmacology that shapes tapering also helps explain why recovery afterward is non-linear.
On top of that slow readaptation, day-to-day life modulates how symptoms feel. A poor night’s sleep, an infection, a stressful event, alcohol, hormonal shifts, or even a large caffeine dose can each tip a good stretch into a wave temporarily. This is one reason a wave can arrive with no change in medication at all — the underlying trajectory is still improving, but a stressor has amplified the symptoms you happen to have that week. Recognizing these modulators is empowering: it reframes a wave from “I’m broken” to “my nervous system is more sensitive to stress right now, and this is likely to pass.”
Why does a wave feel like relapse — and how can you tell the difference?
This is the psychological trap at the center of windows and waves. After a good window, a wave can feel catastrophic — proof that the original condition is roaring back, or that the medication caused permanent damage. That interpretation is understandable and, for many people, wrong. Framer observed that across roughly 6,000 case histories, “clinicians often mistake withdrawal symptoms for relapse,” creating “a trail of such misdiagnosis from multiple prescribers” (2021). The cost of that mistake is real: a withdrawal wave read as relapse can lead to the medication being restarted at full dose or a new drug added, when the wave might have settled on its own.
So how do you tell them apart? You often can’t do it with certainty in the moment — which is exactly why this belongs in a conversation with your prescriber. But clinicians who study the distinction point to a few practical clues. Horowitz and Taylor (BJPsych Advances, 2022) note that “withdrawal symptoms usually occur days after reducing or stopping an antidepressant, whereas relapse might be expected to occur weeks, months or years later.” They also emphasize symptom quality: withdrawal tends to combine physical symptoms (nausea, dizziness, “electric zaps” in the head) with emotional ones, and it typically resolves quickly — often within about a week — if the previous dose is reinstated, whereas relapse follows a slower course.
| Clue | Points toward withdrawal | Points toward relapse |
|---|---|---|
| Timing after a dose change | Days | Usually weeks to months |
| Physical symptoms (dizziness, nausea, brain zaps) | Common, mixed with mood symptoms | Uncommon |
| Onset pattern | Rapid, “wave-like,” peaks then eases | Gradual build-up |
| Response to reinstating the prior dose | Often improves within about a week | Slower, less immediate |
| Resemblance to original illness | May include new or unfamiliar symptoms | Mirrors the original condition |
These are pattern clues, not a diagnostic test, and the two states genuinely overlap. For a fuller walkthrough, see discontinuation vs relapse. The takeaway for waves specifically: a symptom surge that arrives soon after a dose reduction, mixes physical and emotional features, and comes in a wave-like burst is more consistent with withdrawal than with your original illness returning.
What does the evidence actually say about waves and protracted symptoms?
Being honest about evidence strength matters in this area. Here is the landscape, from strongest to most observational.
Withdrawal is common and can be severe. A 2019 systematic review (Davies & Read, Addictive Behaviors, 97:111–121) found that about 56% of people who come off antidepressants experience withdrawal effects, and 46% of those describe them as severe. This is a review of many studies of varying quality, and its exact figures have been debated, but the core conclusion — withdrawal is frequent and not trivial — is now reflected in mainstream guidance.
Duration is variable, and usually shorter than people fear. The UK’s NICE guideline on depression (NG222, 2022) states that withdrawal symptoms often appear within days of a dose reduction and “usually go away within 1 to 2 weeks,” but can sometimes last several weeks and occasionally several months. For most people, the wave pattern belongs to a bounded stretch of recovery rather than an open-ended state.
A minority experience protracted withdrawal. The longest waves belong to what researchers call protracted withdrawal syndrome. In a descriptive analysis of 69 detailed reports drawn from a large online forum (Hengartner et al., Therapeutic Advances in Psychopharmacology, 2021), self-reported protracted symptoms lasted a median of about 26 months (mean 37, range 5–166 months). This is important context, but note the evidence type: these are self-selected consumer narratives from an internet forum, which the authors are explicit about. People with the hardest, longest courses are more likely to seek out and post in such forums, so this describes the severe tail of the distribution, not the average experience. It tells us protracted withdrawal is real for some; it does not tell us how likely it is for any given person.
The “windows and waves” pattern itself is community-originated. It was named and documented by patients — the Surviving Antidepressants community maintains dedicated documentation of “The Windows and Waves Pattern of Stabilization” — and later adopted by deprescribing-focused clinicians such as Framer and Horowitz. Treat it as a credible lived-experience framework that clinicians now use, not as a validated clinical endpoint.
How does tracking a wave help you get through it?
The cruelest feature of a wave is that, while you are in one, it is very hard to believe you were ever well — and while you are in a window, it is easy to forget how bad the last wave was. Memory bends toward your current state. That is precisely where a written record earns its keep.
When you log symptoms, sleep, and dose day by day, two things become visible that feelings alone hide. First, you can see that windows exist at all — a solid week two months ago is undeniable evidence that your nervous system can produce good days. Second, over time you can often see the trend the pattern predicts: waves getting shorter and less intense while windows lengthen. Seeing that trajectory on paper is a direct antidote to catastrophizing, because it replaces “this is permanent” with “the last three waves lasted 9, 6, and 4 days.” Community documentation and clinicians who use this framework consistently describe the same encouraging direction of travel, even though the line is jagged rather than smooth.
This is one place a diary app earns its place. RxDown is built for exactly this: a quick daily log of symptoms, mood, and sleep alongside your dose, a taper calculator for planning gentle reductions, and a doctor report you can bring to an appointment so a wave is a shared data point rather than a panicked description. The goal is not more screen time — it is turning an invisible, memory-distorted process into something you and your prescriber can actually see. You can track this on paper just as well; the point is that something records the pattern.
What should you do during a wave?
The instinct during a wave is to do something drastic — cut faster to “get it over with,” or reach for a new medication. The approaches most often described by deprescribing clinicians and patient communities point the other way: steady the ship, and postpone big decisions until you can see clearly again.
- Hold, don’t cut, during a wave. Many tapering protocols advise pausing further dose reductions — “holding” at the current dose — until symptoms settle, rather than reducing again in the middle of a wave. Reducing further while already destabilized tends to compound the wave. See hold and reinstate for how holding and, if needed, reinstatement are used.
- Don’t make taper decisions mid-wave. A wave is the worst moment to judge whether the whole plan is failing, because everything feels hopeless inside one. Note what is happening, and revisit the plan with your prescriber once you reach a window.
- Protect the basics — especially sleep. Since poor sleep, stress, alcohol, and illness can each amplify a wave, the highest-yield moves are unglamorous: regular sleep, reduced stress load, limiting alcohol and excess caffeine, and gentle routine. See sleep during withdrawal for practical strategies.
- Name the symptom. Recognizing a specific symptom as a known withdrawal effect — for example, that brain zaps are a documented, self-limiting withdrawal phenomenon — reduces the fear that amplifies it.
None of this involves changing your dose on your own. Holding, reducing, and reinstating are all decisions to make with your prescriber; this section describes published approaches and their rationale, not instructions for a specific dose.
When does a prolonged wave warrant a clinical review?
Most waves settle. Some situations, though, call for prompt contact with your prescriber or clinician rather than waiting it out:
- A wave that keeps intensifying over weeks instead of easing, or that is more severe than any previous wave.
- Symptoms that impair function — you can’t work, sleep, or care for yourself — or that don’t fit the withdrawal pattern you’ve come to recognize.
- New or unfamiliar symptoms, especially neurological ones, or anything that could have another medical cause; a wave is not a reason to skip evaluating a genuinely new problem.
- Any thoughts of self-harm or suicide. This is an emergency — contact your clinician, a crisis line, or emergency services immediately. Do not wait for the wave to pass.
- Uncertainty about withdrawal versus relapse that is affecting your decisions. This is the exact judgment call clinicians are there for, and a written symptom timeline makes that conversation far more productive.
Bringing a record helps here too: a clinician can act on “waves that used to last two weeks are now lasting six and getting worse” far more confidently than on “I feel awful.” For preparing that conversation, see talking to your doctor about deprescribing and our FAQ.
The overarching message of windows and waves is a hopeful one, held honestly: recovery is real but rarely linear, a wave is usually a detour rather than a destination, and the trend over time — visible far more reliably on paper than in the middle of a bad week — is toward longer windows and shorter waves.
Sources
- Framer A. What I have learnt from helping thousands of people taper off antidepressants and other psychotropic medications. Therapeutic Advances in Psychopharmacology (2021).
- Horowitz MA, Taylor D. Tapering of SSRI treatment to mitigate withdrawal symptoms. The Lancet Psychiatry (2019).
- Horowitz MA, Taylor D. Distinguishing relapse from antidepressant withdrawal: clinical practice and antidepressant discontinuation studies. BJPsych Advances (2022).
- Davies J, Read J. A systematic review into the incidence, severity and duration of antidepressant withdrawal effects: Are guidelines evidence-based? Addictive Behaviors (2019).
- Hengartner MP, et al. Protracted withdrawal syndrome after stopping antidepressants: a descriptive quantitative analysis of consumer narratives from a large internet forum. Therapeutic Advances in Psychopharmacology (2021).
- Surviving Antidepressants. The Windows and Waves Pattern of Stabilization (patient-community documentation).
- NICE. Depression in adults: treatment and management (NG222) — Recommendations (2022).
Frequently asked questions
What is the difference between a window and a wave in withdrawal?
A window is a period — hours, days, or weeks — when withdrawal symptoms ease or disappear and you feel close to your old self. A wave is a return or intensification of symptoms that follows. Most people who describe this pattern report that windows and waves alternate irregularly rather than following a fixed schedule.
How do I know if a wave is withdrawal or a relapse of my original condition?
Timing and symptom quality are the main clues. Withdrawal typically appears within days of a dose change and mixes physical symptoms (dizziness, nausea, 'brain zaps') with emotional ones, whereas relapse usually builds gradually over weeks to months and mirrors your original illness. Because the two overlap, this is a decision to make with your prescriber rather than alone.
Do waves really get shorter over time?
In the patient-community and clinical accounts that describe this pattern, windows tend to lengthen and waves tend to shorten and soften as the nervous system readapts. This trajectory is uneven, not a smooth curve, and timelines vary widely between people. Keeping a written record is the most reliable way to see the trend, because memory is biased toward whichever state you are in right now.
Tracking your dose, sleep, and symptoms makes every conversation in this article easier. RxDown is a free diary built for exactly that. Get RxDown · Free taper calculator