Hyperbolic Tapering: Why Proportional Cuts Beat Fixed Ones
⚕️ This article is education, not medical advice. Every claim is sourced below. Never stop or change medication without your prescriber — some medications are dangerous to stop abruptly.
TL;DR: Hyperbolic tapering means reducing a medication by a proportion of the current dose rather than by the same fixed number of milligrams each time, so the size of each cut shrinks as the dose gets lower. This mirrors pharmacology: brain receptor occupancy changes very little when you cut a high dose but changes steeply near the bottom, so equal milligram cuts hit harder and harder as you taper down. Making the reductions proportional keeps each step’s effect on the brain roughly even, which is why the Maudsley Deprescribing Guidelines and updated NICE and Royal College of Psychiatrists advice all endorse slow, proportionate, symptom-led reductions. It is not faster than a fixed taper—usually slower—but it is designed to make stopping more tolerable.
This article is education, not medical advice. It describes published approaches and dose ranges from the research literature; it does not tell you what to take. Any change to your medication should be planned and supervised by your prescriber, and medication should never be stopped abruptly. Individual needs vary widely.
What is hyperbolic tapering?
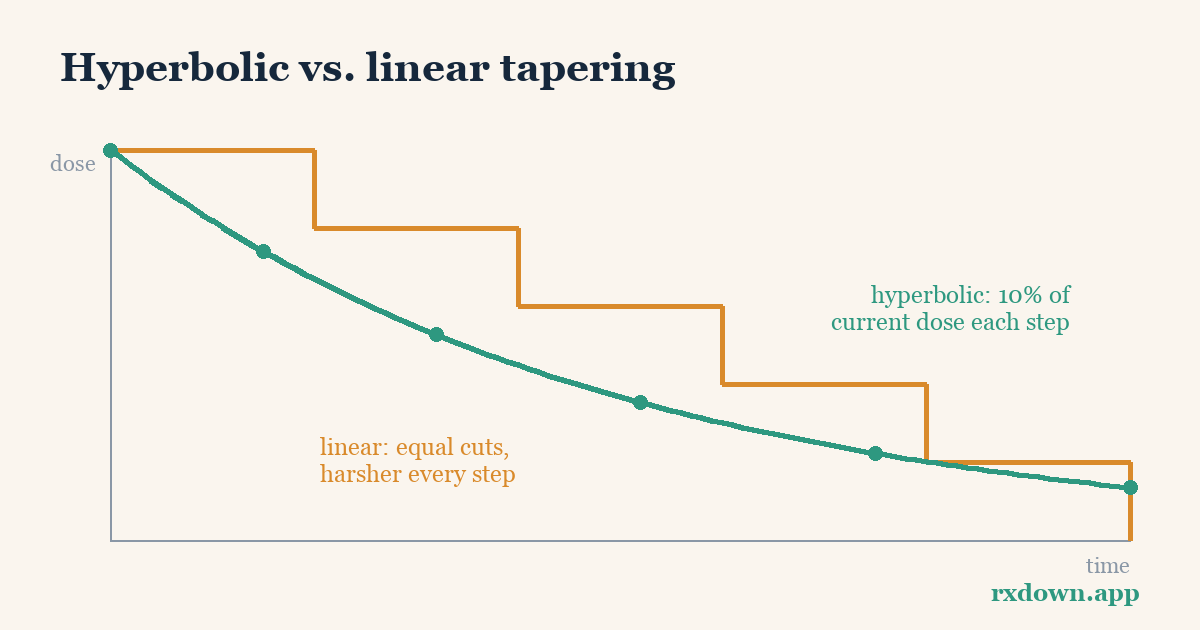
Hyperbolic tapering is a way of reducing a medication in which each step removes a set proportion of the most recent dose instead of a set number of milligrams. Because you are always cutting a percentage of what is left, the absolute amount removed gets progressively smaller as the dose falls. A schedule plotted on a graph traces a curve that drops quickly at first and then flattens into a long, shallow tail toward zero—the shape mathematicians call hyperbolic.
The term was popularized by psychiatrist-researchers Mark Horowitz and David Taylor in a 2019 paper in Lancet Psychiatry on tapering SSRIs. Their central argument is that a taper should be designed around the drug’s effect on the brain, not around round numbers of milligrams. The same idea has long been implicit in how clinicians withdraw benzodiazepines; the 2019 work made the pharmacological rationale explicit for antidepressants and provided a framework that has since been extended to other drug classes.
The practical consequence is that a hyperbolic taper has many small steps at the low end. Getting from a therapeutic dose down to half of it may be relatively easy; getting from a small dose down to zero is where most people need the finest, slowest steps.
Why do equal dose cuts hit harder near the bottom?
The rationale comes from receptor occupancy—how much of a drug’s target the medication is actually blocking or binding at a given dose. For SSRIs, the relevant target is the serotonin transporter (SERT). Positron emission tomography (PET) studies mapped this relationship directly: in a widely cited 2004 study by Meyer and colleagues in the American Journal of Psychiatry, roughly 80% of serotonin transporters were occupied at usual therapeutic doses, with about 77% occupancy measured at 20 mg of citalopram.
The key finding is that the dose–occupancy curve is not a straight line. Occupancy rises steeply at low doses and then plateaus at higher ones. That means:
- Cutting from a high dose to half of it barely moves occupancy—the brain hardly notices, because you are sliding along the flat top of the curve.
- Cutting the same number of milligrams near the bottom produces a large drop in occupancy, because there you are on the steep part of the curve.
So a “steady” taper of, say, 5 mg every few weeks is not steady from the brain’s point of view at all. Early cuts do almost nothing; late cuts of the same size cause the biggest pharmacological changes—right when many people report the worst withdrawal. To make the effect change in even increments, the dose has to be reduced by ever-smaller amounts: a hyperbolic curve. For a deeper walkthrough of the biology, see why receptor occupancy matters.
How big is each step in a hyperbolic taper?
There is no single universal number, but published approaches commonly describe reducing by around 10% of the most recent dose per step, with larger proportional reductions sometimes used higher up and smaller ones toward the end. NICE guidance NG222 (2022) frames it as reducing “in a step-wise fashion, at each step prescribing a proportion of the previous dose (for example, 50% of previous dose),” and using “smaller reductions (for example, 25%) as the dose becomes lower.” The Maudsley Deprescribing Guidelines translate the principle into drug-by-drug schedules that aim for roughly equal reductions in receptor occupancy at each step.
The table below is an illustration of the arithmetic only—not a dosing schedule—to show why proportional cuts behave so differently from fixed ones as the dose falls:
| Illustrative current dose | Fixed cut of 5 mg (share of dose removed) | Proportional cut of ~10% (mg removed) |
|---|---|---|
| 40 mg | 5 mg (about 13%) | 4 mg |
| 20 mg | 5 mg (25%) | 2 mg |
| 10 mg | 5 mg (50%) | 1 mg |
| 5 mg | 5 mg (100% — straight to zero) | 0.5 mg |
| 2.5 mg | not possible with a 5 mg step | 0.25 mg |
| 1 mg | not possible with a 5 mg step | 0.1 mg |
A fixed cut removes a bigger and bigger share of the remaining dose—and of receptor occupancy—the lower you go, until it forces an abrupt jump to zero. A proportional cut keeps that share constant, which is what keeps each step’s impact on the brain roughly even. A hyperbolic taper never quite reaches zero by pure math, so real schedules end with a defined final small step off the lowest achievable dose.
How long should you wait between steps?
Intervals are typically described as 2 to 4 weeks per step, but the pace is meant to be led by symptoms rather than the calendar. The Maudsley Deprescribing Guidelines suggest reductions roughly every 2–4 weeks depending on tolerability, and both NICE and the Royal College of Psychiatrists emphasize that the speed and duration of withdrawal should be agreed with the person and adjusted to how they cope.
In practice this means holding at a dose until any withdrawal symptoms from the last reduction have settled before taking the next step—and pausing, or briefly returning to the previous dose, if a step proves too hard. That “hold” strategy is a normal, planned part of tapering, not a failure; see holding and reinstating during a taper. Because the low-dose steps produce the largest occupancy changes, many people find the intervals need to lengthen toward the end even as the milligram cuts get tiny. A whole taper of a long-term medication may take many months.
Who needs to go slower, and who can go faster?
Tapering is individual, and several factors reliably push toward a slower schedule:
- Longer time on the medication. In the Groot and van Os 2021 tapering-strip cohort, discontinuation success fell with duration of use—about 78% for people who had taken the drug for under a year versus 59% for those on it more than ten years—suggesting long-term users generally need more gradual reductions.
- Short-half-life, higher-potency drugs. Medications such as paroxetine (Paxil, Seroxat) and venlafaxine (Effexor) are associated with more intense discontinuation symptoms and usually warrant slower, finer tapers.
- A history of withdrawal or failed attempts. In the van Os and Groot 2023 analysis of 608 people, 52.5% had previously tried and failed to stop, and those needing the longest tapers were the most likely to have failed before.
Conversely, someone on a long-half-life drug such as fluoxetine (Prozac), which self-tapers as it clears slowly from the body, or someone treated only briefly, may tolerate a faster reduction. The honest summary is that the pace is set by your response, verified step by step with your prescriber—not fixed in advance. Talking this through openly matters; see talking to your doctor about deprescribing.
How do you make tiny doses when tablets don’t split that small?
This is the practical bottleneck of hyperbolic tapering. The final steps often require doses well below the smallest commercial tablet, and ordinary tablets cannot be split accurately into fractions of a milligram. Splitting also can’t be used at all for modified-release, enteric-coated, or capsule products without specific pharmacist guidance. Published solutions include:
- Liquid formulations. Many antidepressants come as an oral solution or suspension, allowing precise small volumes to be measured with an oral syringe. This is the most flexible route for very low doses.
- Tapering strips. Developed and studied by Groot and van Os, these are 28-day rolls of daily pouches in which each pouch contains the same or a slightly lower dose than the one before, letting the dose step down in small, pre-planned increments.
- Compounded doses. A compounding pharmacy can prepare capsules or liquids at custom low strengths where a suitable licensed product does not exist.
The Maudsley Deprescribing Guidelines devote substantial space to these formulation practicalities precisely because the pharmacology only works if the small doses can actually be made. If you are told a taper “isn’t possible” because tablets don’t go low enough, these approaches are worth raising with your prescriber and pharmacist. A taper calculator can help you and your clinician visualize what the low-end steps look like before you commit to a plan.
How does this anchor the Maudsley Deprescribing Guidelines?
Published by Wiley-Blackwell in 2024, The Maudsley Deprescribing Guidelines: Antidepressants, Benzodiazepines, Gabapentinoids and Z-drugs (Horowitz and Taylor) is the first comprehensive professional guideline dedicated to stopping psychiatric medication rather than starting it. Hyperbolic tapering is its organizing principle. The book opens with essays making the pharmacological case—including the distinction between withdrawal and relapse, and the argument for thinking in receptor occupancy rather than milligrams—and then provides detailed, drug-by-drug schedules built to achieve roughly equal occupancy reductions at each step.
Its influence is visible across mainstream guidance. NICE’s NG222 now recommends step-wise reductions by a proportion of the previous dose with smaller cuts as the dose falls, and the Royal College of Psychiatrists’ 2020 patient resource “Stopping antidepressants” advises tapering over “months or longer” in progressively smaller steps, titrated to what the person can tolerate. In other words, the once-fringe idea of proportional, occupancy-based tapering has become the reference framework for safe withdrawal.
How strong is the evidence for hyperbolic tapering?
It is worth being precise about what is and isn’t proven, because this is an active area of debate.
The pharmacological rationale is well established. The hyperbolic dose–occupancy relationship rests on direct PET imaging (Meyer et al., 2004) and is not seriously contested; halving a therapeutic SSRI dose really does change receptor occupancy far less than the same cut near zero.
The clinical outcome data are mostly observational. The strongest real-world support comes from tapering-strip cohorts: across three retrospective studies recruiting more than 2,000 patients, around 70% of people attempting to stop were able to discontinue using hyperbolic tapering strips (Groot and van Os), with a median of two 28-day strips over roughly two months. These are encouraging but observational—people who sought out tapering strips were often highly motivated and had frequently failed with faster methods—so they show feasibility rather than proof of superiority from a randomized trial.
How common and severe withdrawal is remains contested. A 2019 systematic review (Davies and Read, Addictive Behaviors) reported that about 56% of people experience withdrawal symptoms when coming off antidepressants and that nearly half of those describe them as severe. A later meta-analysis (Henssler et al., Lancet Psychiatry, 2024) estimated a lower figure—roughly 15%, about one in six to seven, once placebo and nocebo effects are subtracted—and concluded severe symptoms are relatively uncommon. Both can be partly true: averages hide wide variation, and a minority experience prolonged, disabling withdrawal even if most do not. Note too that patient communities consistently report protracted symptoms that formal trials, often measuring only short follow-up, may underestimate; these community-reported patterns are real signals but are lower-strength evidence than controlled studies. For how symptoms typically evolve over time, see the antidepressant withdrawal timeline, and for telling the two apart, discontinuation versus relapse.
The reasonable takeaway: hyperbolic tapering is a biologically well-grounded, guideline-endorsed strategy to make stopping more tolerable for people who struggle with faster reductions. It is not a guarantee against withdrawal, and it is generally slower, not quicker.
If you’re tracking your own taper, a diary can turn vague impressions into something you and your prescriber can act on. RxDown lets you log doses, symptoms, and sleep day by day, visualize a proportional (hyperbolic) schedule with its built-in taper calculator, and export a concise doctor report so decisions about pace are grounded in your actual data rather than memory. It is a record-keeping tool, not a substitute for medical care.
Have a specific question about pace, formulations, or symptoms? Our frequently asked questions cover many of the common ones.
Sources
- Horowitz MA, Taylor D. Tapering of SSRI treatment to mitigate withdrawal symptoms. Lancet Psychiatry (2019)
- Meyer JH, et al. Serotonin Transporter Occupancy of Five SSRIs at Different Doses: An [11C]DASB PET Study. Am J Psychiatry (2004)
- Horowitz MA, Taylor D. The Maudsley Deprescribing Guidelines: Antidepressants, Benzodiazepines, Gabapentinoids and Z-drugs. Wiley-Blackwell (2024)
- Royal College of Psychiatrists. Stopping antidepressants — patient resource (2020)
- NICE. Depression in adults: treatment and management (NG222) (2022)
- Groot PC, van Os J. Successful use of tapering strips for hyperbolic reduction of antidepressant dose: a cohort study. Ther Adv Psychopharmacol (2021)
- van Os J, Groot PC. Outcomes of hyperbolic tapering of antidepressants. Ther Adv Psychopharmacol (2023)
- Davies J, Read J. A systematic review into the incidence, severity and duration of antidepressant withdrawal effects. Addictive Behaviors (2019)
- Henssler J, et al. Incidence of antidepressant discontinuation symptoms: a systematic review and meta-analysis. Lancet Psychiatry (2024)
Frequently asked questions
What is hyperbolic tapering in simple terms?
It means reducing your medication by a percentage of your current dose rather than by the same fixed amount each time. Because you always cut a proportion of what remains, the absolute reduction gets smaller and smaller as the dose falls. This keeps the effect on the brain roughly even at every step instead of getting harsher near the end.
How much should each hyperbolic step reduce the dose?
Published approaches often describe reductions of around 10% of the most recent dose, with larger proportional cuts (25–50%) sometimes used at higher doses and smaller ones near the bottom. The exact percentage and pace are set with your prescriber and adjusted to how you feel. The goal is roughly equal reductions in receptor occupancy, not equal reductions in milligrams.
Why can't I just split my tablets to taper slowly?
Ordinary tablets rarely divide accurately below a few milligrams, and the smallest commercial dose is often still far too high for the final steps. Prescribers may use liquid formulations, compounded capsules, or tapering strips to make the very small, precise doses a hyperbolic taper requires. Never crush or split a modified-release or enteric-coated product without pharmacist advice.
Tracking your dose, sleep, and symptoms makes every conversation in this article easier. RxDown is a free diary built for exactly that. Get RxDown · Free taper calculator