Know Your Medication: Benzodiazepines vs Z-Drugs vs DORAs
⚕️ This article is education, not medical advice. Every claim is sourced below. Never stop or change medication without your prescriber — some medications are dangerous to stop abruptly.
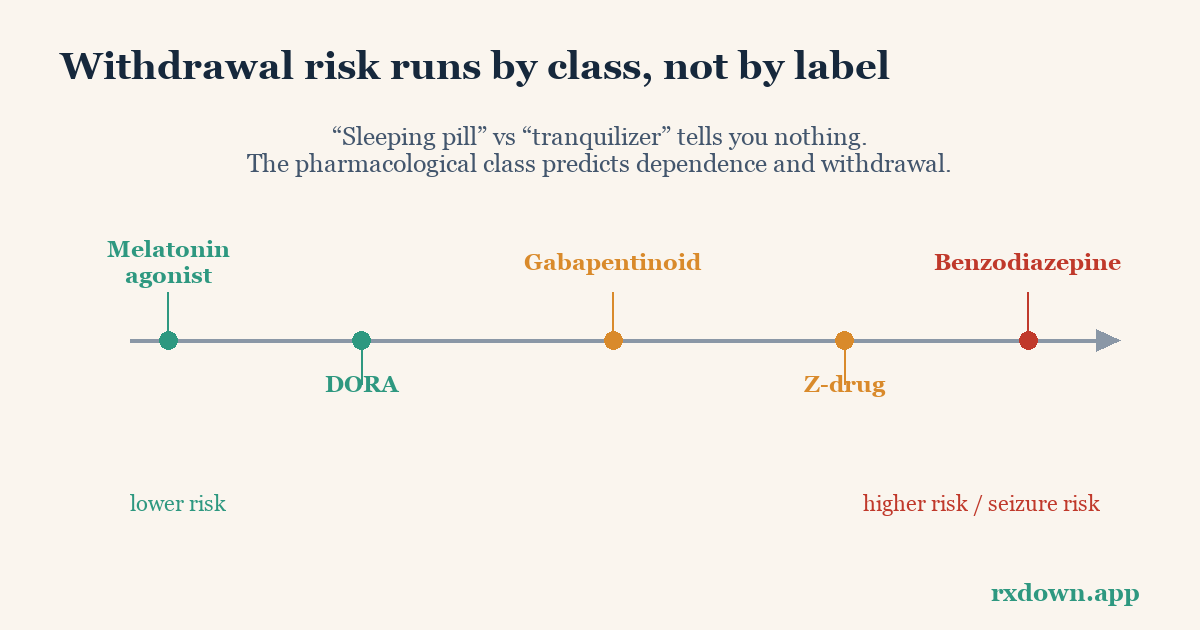
TL;DR: The single most useful thing to know about a sleep or anxiety medication is its class, because the class — not the brand name or what the pill is “for” — predicts how it works and how carefully you have to come off it. Benzodiazepines and Z-drugs both act on the brain’s GABA “brake” and can cause tolerance, dependence, and a withdrawal syndrome, so they usually need a slow taper. Dual orexin receptor antagonists (DORAs) block the brain’s wake signal instead and showed no withdrawal in trials. Melatonin agonists act on the body clock and aren’t controlled substances. This guide shows you how to identify which class you’re taking and why it matters. It is education, not medical advice; confirm your medication with your pharmacist or prescriber, and never stop a GABA-acting drug abruptly.
Why should I care what class my drug is in?
Because two pills that both “help you sleep” can be worlds apart in how they behave when you stop. A drug’s class tells you three things the brand name never will:
- Mechanism — what it does in the brain (amplify the brake, block the accelerator, nudge the clock).
- Dependence and withdrawal risk — whether your body adapts to it, and whether stopping triggers a withdrawal syndrome.
- How to stop — abruptly (rarely safe), or via a slow, individualized taper.
Get the class right and the stopping plan almost writes itself. Get it wrong — assume a “sleeping pill” is harmless when it is actually a benzodiazepine — and an abrupt stop can be dangerous. This is the same reason the sleeping pills vs. sedatives question matters: the label misleads, the class does not.
How do I identify my medication’s class?
The reliable method is simple: find the generic name (the lowercase non-brand name on the label or leaflet) and check it against a class list, or just ask your pharmacist — they will tell you in seconds. Naming patterns can give you a head start, though they are hints, not guarantees:
- Benzodiazepines usually end in -pam or -lam: diazepam, lorazepam, clonazepam, temazepam, alprazolam.
- Z-drugs conveniently start with Z: zolpidem, zopiclone, eszopiclone, zaleplon.
- DORAs end in -orexant: daridorexant, lemborexant, suvorexant.
- Melatonin agonists: ramelteon (and plain melatonin).
Never rely on the pattern alone for a stopping decision — confirm the class before you change anything.
Benzodiazepines: the original sedative-hypnotics
Benzodiazepines are positive allosteric modulators of the GABA-A receptor — they amplify GABA, the brain’s main inhibitory (slow-down) neurotransmitter, producing calm, sleep, muscle relaxation, and reduced anxiety. They are used both for anxiety (“tranquilizers”) and for sleep, and the same molecule can do both depending on dose and timing.
What defines them for stopping purposes:
- The brain adapts to their presence (tolerance), so the same dose does less over time, and stopping unmasks a rebound in the opposite direction.
- They can cause physical dependence and a withdrawal syndrome — anxiety, insomnia, sensory disturbances, and, importantly, a risk of seizures if stopped abruptly from a significant dose.
- Half-life varies enormously, from short-acting (e.g., lorazepam, alprazolam) to long-acting (e.g., diazepam). This matters for tapering, which is why the Ashton approach often substitutes a longer-acting benzodiazepine before stepping down (see the Ashton Manual guide).
Because of these risks, NICE places benzodiazepines squarely among “medicines associated with dependence or withdrawal symptoms.”
Z-drugs: chemically different, functionally similar
Z-drugs (zolpidem/Ambien, zopiclone, eszopiclone/Lunesta, zaleplon/Sonata) were introduced as a cleaner alternative to benzodiazepines. Chemically they are different molecules — but they bind at or near the same benzodiazepine site on the GABA-A receptor, so they share the core risks. As the Ashton Manual puts it, they “act in the same way and have the same adverse effects including dependence and withdrawal reactions.”
Two facts anchor the reality:
- A 2019 review in the International Journal of Neuropsychopharmacology documented genuine Z-drug abuse and dependence potential, particularly at high doses and in people with a history of substance use.
- In 2019 the FDA added a Boxed Warning — its strongest — to certain Z-drugs and older insomnia benzodiazepines because of rare but serious complex sleep behaviors (sleep-walking, sleep-driving) that caused injuries and deaths.
So for stopping purposes, treat Z-drugs like benzodiazepines: usually a taper, never an abrupt stop from regular use. Our Z-drug reduction guide covers this in detail.
DORAs: blocking the wake signal instead
Dual orexin receptor antagonists — daridorexant (Quviviq), lemborexant (Dayvigo), suvorexant (Belsomra) — take the opposite approach. Instead of amplifying the brake, they block orexin, a neuropeptide that keeps you awake. Turn the wake signal down and natural sleep can take over.
This mechanism difference shows up when you stop. In the phase 3 trials and the FDA labels, abruptly stopping a DORA — even after up to 12 months — did not produce rebound insomnia or measurable withdrawal signs. They are still Schedule IV controlled substances, but that reflects abuse-potential studies (drug-liking similar to zolpidem), not evidence of physical dependence. The full picture is in the DORA discontinuation guide.
What about melatonin agonists, sedating antidepressants, and antihistamines?
Several other drugs are used for sleep or anxiety and are worth recognizing:
- Melatonin agonists (ramelteon/Rozerem, melatonin). Ramelteon acts on the body-clock melatonin receptors, has no meaningful affinity for the sedation receptors, is the only prescription insomnia drug not scheduled by the DEA, and has not been linked to dependence or withdrawal.
- Sedating antidepressants used off-label for sleep (trazodone, mirtazapine, low-dose doxepin). These are antidepressants, so they don’t cause GABA-type dependence, but they can produce antidepressant discontinuation effects if stopped quickly.
- Sedating antihistamines (diphenhydramine, doxylamine) — the usual ingredients in over-the-counter “PM” sleep aids. Tolerance to their sleep effect develops quickly, and they carry their own risks (especially anticholinergic effects in older adults).
- Gabapentinoids (gabapentin, pregabalin), sometimes used for anxiety or sleep, are also on NICE’s dependence/withdrawal list and need a planned taper.
The class-by-class comparison
| Class | Examples | How it works | Controlled substance? | Dependence / withdrawal | Usually needs a taper? |
|---|---|---|---|---|---|
| Benzodiazepines | diazepam, lorazepam, alprazolam, temazepam | Amplify GABA (brake) | Yes (Schedule IV, US) | Yes — incl. seizure risk if abrupt | Yes |
| Z-drugs | zolpidem, zopiclone, eszopiclone | Amplify GABA at the same site | Yes (Schedule IV, US) | Yes — tolerance, rebound, withdrawal | Yes |
| DORAs | daridorexant, lemborexant, suvorexant | Block orexin (accelerator) | Yes (Schedule IV, US) | Not seen in trials | Not for withdrawal reasons |
| Melatonin agonists | ramelteon, melatonin | Act on body-clock receptors | No (ramelteon unscheduled) | Not associated | No |
| Sedating antidepressants | trazodone, mirtazapine, doxepin | Various (histamine/serotonin) | No | Antidepressant discontinuation effects | Yes, if long-term |
| Gabapentinoids | gabapentin, pregabalin | Calcium-channel modulation | Pregabalin scheduled (US) | Yes (on NICE list) | Yes |
Controlled-substance scheduling reflects US classification and can differ by country.
The bottom line
Before you think about anxiety about stopping, dose changes, or side effects, answer one question: what class is my medication? Benzodiazepines and Z-drugs are GABA-acting sedative-hypnotics that can cause dependence and a withdrawal syndrome, so they need a careful, prescriber-supervised taper. DORAs block the wake signal and melatonin agonists act on the clock — neither showed a withdrawal syndrome. Find your drug’s generic name, confirm the class with your pharmacist, and let the class shape the plan. When you’re ready, when and how to start tapering explains the methods, and the taper calculator can sketch a schedule to discuss with your prescriber. See also the FAQ.
Sources
- Anxiolytics and Sedative-Hypnotics Toxicity, StatPearls, NCBI Bookshelf (2023)
- Ashton CH, Benzodiazepines: How They Work and How to Withdraw (The Ashton Manual, 2002/rev. 2011)
- U.S. FDA, Boxed Warning for Certain Prescription Insomnia Medicines (2019)
- Schifano F et al., An Insight into Z-Drug Abuse and Dependence, International Journal of Neuropsychopharmacology (2019)
- Mignot E, et al., Safety and efficacy of daridorexant in adults with insomnia disorder, Lancet Neurology (2022)
- QUVIVIQ (daridorexant) Prescribing Information, FDA (2022)
- Simpson D, Curran MP, Ramelteon: A Review of its Use in Insomnia, Drugs / PMC (2008)
- NICE, Medicines associated with dependence or withdrawal symptoms (NG215) (2022)
Frequently asked questions
How do I find out what class my medication is in?
Look at the generic name (not the brand) on the label, then check it against a class list or ask your pharmacist — that is the fastest reliable answer. As rough signals: benzodiazepine generic names often end in '-pam' or '-lam' (diazepam, lorazepam, alprazolam); Z-drug names start with Z (zolpidem, zopiclone, zaleplon); DORAs end in '-orexant' (daridorexant, lemborexant, suvorexant). These are patterns, not rules, so confirm with a pharmacist or your prescriber rather than guessing.
Why does the drug class matter so much?
Because the class predicts whether stopping causes a physical withdrawal syndrome and how the drug should be tapered. Benzodiazepines and Z-drugs act on GABA and can cause tolerance, dependence, and withdrawal — including, for benzodiazepines, seizure risk — so they usually need a slow taper. DORAs and melatonin agonists were not associated with withdrawal in trials. The class, not the brand name or what the drug is 'for,' is what shapes a safe stopping plan.
Are Z-drugs really safer than benzodiazepines?
They were marketed that way, but pharmacologically the difference is smaller than the marketing implied. Z-drugs act on the same GABA-A receptor system as benzodiazepines and can cause tolerance, dependence, rebound insomnia, and withdrawal. In 2019 the FDA added a Boxed Warning to certain Z-drugs and older insomnia benzodiazepines for rare but serious complex sleep behaviors. Treat them as close relatives, not a risk-free alternative.
Tracking your dose, sleep, and symptoms makes every conversation in this article easier. RxDown is a free diary built for exactly that. Get RxDown · Free taper calculator