Antidepressant Withdrawal Timeline: Symptoms & Duration
⚕️ This article is education, not medical advice. Every claim is sourced below. Never stop or change medication without your prescriber — some medications are dangerous to stop abruptly.
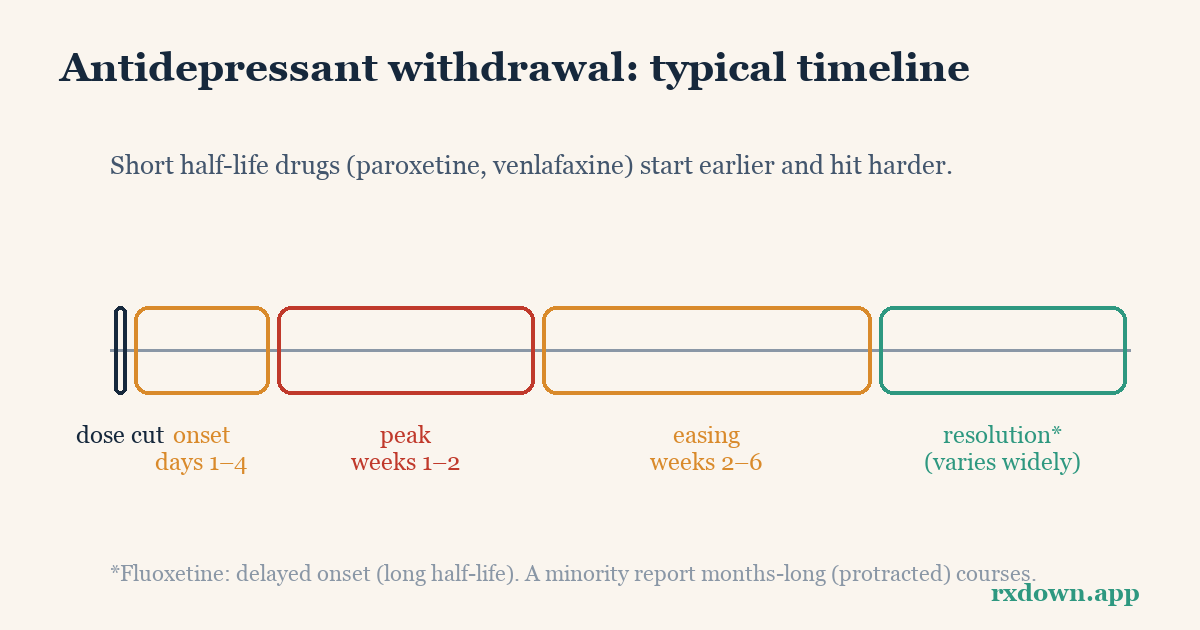
TL;DR: Antidepressant withdrawal (also called discontinuation) symptoms most often begin 1–4 days after a dose is lowered or missed, with fluoxetine’s onset delayed because it leaves the body slowly. Common symptoms follow the FINISH pattern — flu-like feelings, insomnia, nausea, imbalance/dizziness, sensory disturbances (including “brain zaps”), and hyperarousal such as anxiety. Estimates of how many people are affected range from about 15% in randomized-trial data to 56% in survey-based reviews, and roughly 3–46% of those affected describe symptoms as severe. Most acute symptoms ease within weeks with a gradual taper, but a minority last months, so any reduction should be planned and supervised with your prescriber.
This article is education, not medical advice. It describes published research and professional guidance so you can have a better-informed conversation with your prescriber. Do not stop or change an antidepressant abruptly. Any dose change should be planned and supervised by the clinician who prescribed it.
How common is antidepressant withdrawal?
Estimates vary a lot depending on how the question is studied, and it helps to see the range honestly.
A widely cited 2019 systematic review (Davies & Read, Addictive Behaviors) pooled 14 studies and found withdrawal incidence ranging from 27% to 86%, with a weighted average of 56%. Across four studies that rated severity, a weighted average of 46% of those with withdrawal described their symptoms as severe. These figures come largely from surveys and observational studies, which tend to capture people who chose to stop and may over-represent difficult experiences.
A large 2024 systematic review and meta-analysis (Henssler et al., The Lancet Psychiatry) took a different approach, analyzing 79 studies and 21,002 patients and subtracting the symptoms reported by people stopping placebo. It found that about one in three people stopping an antidepressant reported symptoms, but after accounting for nonspecific (nocebo) effects, roughly 15% — about one in six to seven — had discontinuation symptoms attributable to the drug itself, and about 3% (one in 35) had symptoms rated as severe.
Both numbers are “true” in their own frame: randomized-trial data give a more conservative attributable estimate, while real-world surveys capture the lived difficulty of coming off. Earlier reviews by Fava and colleagues (2015 for SSRIs, 2018 for SNRIs, Psychotherapy and Psychosomatics) concluded that withdrawal reactions affect roughly 30–60% of users depending on method and drug. The practical takeaway: withdrawal is common enough to plan for, and its severity is unpredictable for any one person.
When do antidepressant withdrawal symptoms start?
For most antidepressants, symptoms appear quickly after a dose is lowered, missed, or stopped. The classic American Family Physician review (Warner et al., 2006) notes that discontinuation symptoms typically appear within about three days, and can begin within hours of a missed dose for short-acting drugs. The FINISH framework (Berber, 1998) describes onset within roughly 2–4 days.
The main exception is fluoxetine (Prozac). Because fluoxetine and its active metabolite norfluoxetine clear the body slowly, the effective dose tapers itself for weeks. Onset is often delayed — sometimes not appearing for one to several weeks — and symptoms tend to be milder. This slow self-taper is also why fluoxetine is sometimes used as a “bridge” during deprescribing under medical supervision.
Timing matters for interpretation. Symptoms that begin within days of a dose change point strongly toward withdrawal rather than a returning illness — a distinction covered in discontinuation vs relapse.
What do antidepressant withdrawal symptoms feel like?
Clinicians often use the FINISH mnemonic (Berber, 1998) to remember the six symptom clusters:
- F — Flu-like symptoms: fatigue, headache, muscle aches, sweating, chills.
- I — Insomnia: trouble sleeping, often with vivid or disturbing dreams.
- N — Nausea: sometimes with vomiting, cramping, or diarrhea.
- I — Imbalance: dizziness, light-headedness, vertigo, unsteady walking.
- S — Sensory disturbances: “brain zaps” (brief electric-shock sensations in the head), tingling, numbness, visual trails. See brain zaps for what they are and why they happen.
- H — Hyperarousal: anxiety, agitation, irritability, and sometimes akathisia (an intense inner restlessness).
Beyond FINISH, people frequently report low or unstable mood, tearfulness, difficulty concentrating, and heightened emotional reactivity. Symptoms tend to be worse with drugs that leave the body quickly (see the half-life table below) and after longer or higher-dose treatment. Because several of these overlap with depression and anxiety symptoms, the pattern and timing — physical symptoms arriving fast after a dose change — are what usually mark them as withdrawal.
Does the drug’s half-life change withdrawal?
Yes — this is one of the most reliable predictors. Half-life is roughly how long it takes the body to clear half a dose. Drugs with a short half-life produce faster, often sharper withdrawal because blood levels fall quickly between doses; drugs with a long half-life taper themselves more gently. The table below draws on published pharmacokinetic values summarized in the American Family Physician review (Warner et al., 2006).
| Antidepressant (brand) | Approx. half-life | Relative withdrawal risk |
|---|---|---|
| Paroxetine (Paxil) | ~21 hours | Higher |
| Venlafaxine (Effexor) | ~5 hours (metabolite ~11 h) | Higher |
| Duloxetine (Cymbalta) | ~11–16 hours | Higher |
| Sertraline (Zoloft) | ~26 hours | Moderate |
| Escitalopram (Lexapro) | ~27–32 hours | Moderate |
| Citalopram (Celexa) | ~35 hours | Moderate |
| Mirtazapine (Remeron) | ~20–40 hours | Lower–moderate |
| Fluoxetine (Prozac) | ~4–6 days (metabolite ~1–2 weeks) | Lower (delayed onset) |
Paroxetine and venlafaxine are consistently flagged as the highest-risk of the commonly prescribed antidepressants, while fluoxetine is lowest-risk for acute withdrawal because of its long tail. This is descriptive pharmacology, not a dosing recommendation — the right medication and schedule for any individual is a decision for the prescriber.
How long does antidepressant withdrawal last?
For many people, acute symptoms build over a few days, peak, and settle within 1–3 weeks, particularly when the reduction is gradual. The 2006 AFP review notes untreated symptoms are usually mild and resolve in one to two weeks; severe symptoms often ease within days if the previous dose is reinstated.
But the honest picture is broader. Davies & Read (2019) concluded it is “not uncommon” for withdrawal to last several weeks or months. The Fava SNRI review (2018) found symptoms can persist for weeks even with gradual tapering, sometimes with late onset. In 2020, the UK Royal College of Psychiatrists updated its patient guidance to acknowledge that while withdrawal is mild and short for some, for others it can be “severe and protracted, lasting for weeks, months or beyond.”
At the far end sits protracted withdrawal. A 2020 analysis (Hengartner et al., Therapeutic Advances in Psychopharmacology) examined patient narratives from a large online forum and described cases lasting months to years — one reported case ran to roughly 69 months. It is important to label this evidence honestly: it comes from patient-community reports, not controlled trials, so it cannot tell us how common protracted withdrawal is. What it does establish is that long courses are real and worth taking seriously.
Recovery is also rarely linear. Many people describe symptom-free “windows” alternating with rougher “waves” rather than a steady improvement — a pattern explored in windows and waves recovery.
Is it withdrawal or is my depression coming back?
This is one of the hardest questions during a taper, and getting it wrong in either direction has costs. A few distinguishing features from professional guidance (RCPsych; clinical reviews):
- Timing: withdrawal appears within days of a dose change; relapse usually builds gradually over weeks to months.
- Symptom type: withdrawal often includes physical symptoms — dizziness, brain zaps, nausea, flu-like feelings — that are not typical of a depressive episode.
- Response to dose: withdrawal usually improves within hours to days if the previous dose is restored; relapse would not reverse that quickly.
- Familiarity: relapse tends to reproduce your original symptoms, whereas withdrawal can feel new or different.
Because the two can overlap and coexist, this is a judgment to make with your prescriber, not alone. The discontinuation vs relapse guide goes deeper, and talking to your doctor about deprescribing can help you frame the conversation.
What are the red flags that need prompt medical attention?
Most withdrawal is uncomfortable but not dangerous. Some situations, however, warrant contacting your prescriber promptly — or seeking urgent care:
- New or worsening thoughts of suicide or self-harm. Seek emergency help immediately (in the US, call or text 988). This is never something to wait out alone.
- Severe agitation, akathisia, or a sense of losing control that you cannot manage.
- Symptoms so severe you cannot function — unable to work, eat, sleep, or care for yourself.
- Symptoms that keep worsening rather than stabilizing, or that persist well beyond what you expected.
- Symptoms after an abrupt stop. Stopping suddenly is the most common trigger for severe withdrawal; tell your prescriber so they can advise on reinstating and tapering more slowly.
- Anything that seems unlike withdrawal — high fever, confusion, chest pain, severe headache unlike your usual — which may point to another cause needing assessment.
A common, evidence-supported response to severe withdrawal is to reinstate the last tolerated dose under medical guidance and then reduce more slowly; the hold and reinstate guide explains this approach. Do not improvise dose changes on your own.
How is antidepressant withdrawal reduced or managed?
The single biggest lever is how slowly the dose comes down. In an influential 2019 paper (Horowitz & Taylor, The Lancet Psychiatry), the authors argued that because the relationship between dose and receptor effect is curved rather than linear, reductions should be hyperbolic — smaller and smaller absolute steps as the dose gets low — to keep each step’s biological impact roughly even. This often means final doses far below the smallest available tablet and a taper measured in months, not days. The reasoning is explained in hyperbolic tapering and the underlying pharmacology in receptor occupancy explained.
Other supported strategies include pausing (holding) at a dose until symptoms settle before the next reduction, and — for very short half-life drugs — sometimes switching to a longer-acting option before tapering, always under a prescriber’s direction. You can explore step sizes and schedules with the taper calculator, and find more common questions in the FAQ.
Tracking symptoms day to day makes all of this easier to steer. RxDown is a private withdrawal diary that lets you log dose changes, sleep, and how you feel, then generate a clear doctor report and model reductions with its taper calculator — so the decision about pace stays a shared, evidence-informed one between you and your prescriber.
Sources
- Davies J, Read J. A systematic review into the incidence, severity and duration of antidepressant withdrawal effects. Addictive Behaviors (2019)
- Henssler J, et al. Incidence of antidepressant discontinuation symptoms: a systematic review and meta-analysis. The Lancet Psychiatry (2024)
- Horowitz MA, Taylor D. Tapering of SSRI treatment to mitigate withdrawal symptoms. The Lancet Psychiatry (2019)
- Warner CH, et al. Antidepressant Discontinuation Syndrome. American Family Physician (2006)
- Berber MJ. FINISH: remembering the discontinuation syndrome. J Clin Psychiatry (1998)
- Fava GA, et al. Withdrawal Symptoms after SSRI Discontinuation: A Systematic Review. Psychotherapy and Psychosomatics (2015)
- Fava GA, et al. Withdrawal Symptoms after SNRI Discontinuation: Systematic Review. Psychotherapy and Psychosomatics (2018)
- Hengartner MP, et al. Protracted withdrawal syndrome after stopping antidepressants. Therapeutic Advances in Psychopharmacology (2020)
- Royal College of Psychiatrists. Stopping antidepressants (patient information)
Frequently asked questions
How soon after stopping an antidepressant do withdrawal symptoms start?
For most short half-life antidepressants, symptoms begin within 1–4 days of a dose reduction or missed dose. Fluoxetine is the main exception: because it and its active metabolite clear slowly, onset can be delayed by one to several weeks, and symptoms are often milder. Any symptom that appears within days of a dose change is more likely to be withdrawal than relapse.
How long does antidepressant withdrawal last?
Many people find acute symptoms ease within a few weeks, especially with a slow taper. Systematic reviews and professional guidance note that some people experience symptoms lasting weeks to months, and patient-community reports describe protracted courses. Duration varies widely by drug, dose, how long it was taken, and how quickly it was reduced.
Is it withdrawal or is my depression relapsing?
Withdrawal usually appears within days of a dose change, features physical symptoms like dizziness and brain zaps, and often improves quickly if the previous dose is restored. Relapse tends to build gradually over weeks and reproduces your original depression. If you are unsure, this is an important thing to discuss with your prescriber rather than deciding alone.
Tracking your dose, sleep, and symptoms makes every conversation in this article easier. RxDown is a free diary built for exactly that. Get RxDown · Free taper calculator