Antidepressant withdrawal vs relapse: how to tell
⚕️ This article is education, not medical advice. Every claim is sourced below. Never stop or change medication without your prescriber — some medications are dangerous to stop abruptly.
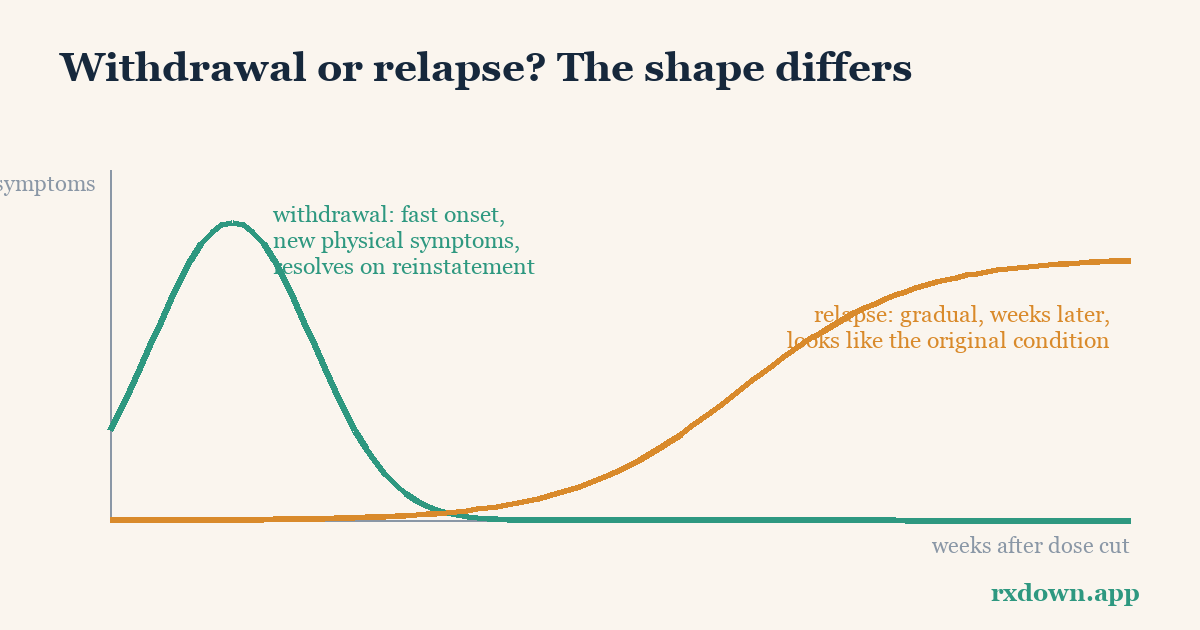
TL;DR: When symptoms come back after you cut an antidepressant dose, there are three practical clues to whether it is withdrawal or a relapse of your original condition. Withdrawal usually starts within days of the change, often includes novel physical symptoms (dizziness, nausea, “brain zaps”) that were never part of your depression or anxiety, and typically eases within days once the dose is restored. Relapse tends to build gradually over weeks to months, mirrors your original illness, and does not resolve quickly with a single dose adjustment. This distinction matters because it points to opposite responses: slow the taper for withdrawal, reconsider treatment for relapse.
This article is education, not medical advice. It describes published approaches and ranges, not a plan for you. Do not stop or change an antidepressant abruptly, and make any dose change together with the prescriber who knows your history. If you feel unsafe or have thoughts of harming yourself, seek urgent help immediately.
Why does telling them apart change anything?
Because withdrawal and relapse call for opposite responses. If returning symptoms are withdrawal, the answer is usually to go back to the last comfortable dose and then reduce more slowly next time. If they are a relapse of the underlying condition, the conversation shifts toward whether to restart or continue treatment, adjust it, or add other support. Get the call wrong in the direction of “relapse” and a person may be told they need the drug indefinitely when they actually needed a gentler taper.
This is not a fringe worry. Mark Horowitz and David Taylor, in a 2022 review in BJPsych Advances, argue that withdrawal has historically been misread as relapse, which inflated apparent relapse rates and made antidepressants look more essential for long-term maintenance than the evidence supports. Keeping the two apart is therefore both a personal clinical decision and a piece of getting the wider evidence right. (We unpack that trial argument below, along with honest counterpoints.)
What is the difference between withdrawal, rebound, and relapse?
Three words get tangled together. They are not the same thing, and clinicians use them precisely:
- Withdrawal (discontinuation) symptoms are the body’s reaction to the drug leaving the system. They can include symptoms you never had before, and they follow the dose change, not the calendar of your illness.
- Rebound is a brief, intense return of the original symptoms right after stopping, often stronger than baseline but short-lived. It is most discussed with sleep medications and benzodiazepines (see z-drugs dependence reduction).
- Relapse is the genuine return of the underlying depressive or anxiety disorder after a period of being well. It reflects the illness itself, not the pharmacology of stopping.
Withdrawal is common. A 2019 systematic review by Davies and Read (Addictive Behaviors, 97:111-121) found that around 56% of people coming off antidepressants experienced withdrawal effects, and of those, roughly 46% rated them as severe. The Royal College of Psychiatrists puts the incidence more conservatively, stating that between a third and a half of people will experience withdrawal to some degree. Either way, this is a normal physiological event, not a sign of weakness or of “needing the drug forever.”
What are the three classic ways to tell withdrawal from relapse?
Clinicians lean on three discriminators: timing, symptom character, and response to reinstatement. No single one is definitive, but together they usually point clearly one way. The table summarizes them; the sections after explain each.
| Feature | Points to withdrawal | Points to relapse |
|---|---|---|
| Timing after a dose change | Starts within days (often 1-5 days) | Emerges gradually over weeks to months |
| Physical symptoms | Common and often novel: dizziness, nausea, “brain zaps,” flu-like feelings | Uncommon; mainly the mood/anxiety of the original illness |
| Symptom character | New physical symptoms mixed with psychological ones | Closely resembles the original episode |
| Trajectory | Rises then falls in a wave (crescendo then decrescendo) | Tends to persist or steadily worsen |
| Response to restoring the dose | Usually improves within days, often within a week | Little or slow change over days |
Source pattern drawn from Horowitz & Taylor (BJPsych Advances, 2022) and Royal College of Psychiatrists guidance.
How fast do withdrawal symptoms start after a dose cut?
Timing is the first and often clearest clue. Withdrawal is tied to the drug’s exit from your system, so it tends to appear within a few days of a reduction or stop, typically one to five days. The Royal College of Psychiatrists describes a characteristic wave: onset a few days after the reduction, worsening to a peak within a couple of weeks, then easing.
Relapse behaves differently. A true return of depression or anxiety usually builds gradually over weeks, months, or longer — it is not triggered by a specific dose change on a specific Tuesday. If your symptoms flared two days after a cut, timing favors withdrawal. If they crept back a couple of months after you finished tapering, with no clear link to a dose change, that pattern is more consistent with relapse.
One important exception: fluoxetine (Prozac) has an unusually long half-life (its active metabolite lingers for one to two weeks), so its withdrawal can be delayed and blunted. With long-half-life drugs, “days” can stretch to a week or two, and the timing clue is less sharp. Our antidepressant withdrawal timeline covers how half-life shapes onset.
Do withdrawal symptoms feel different from my original depression?
Often, yes — and this is the second discriminator. Withdrawal frequently produces physical and “novel” symptoms that were never part of the original condition. Classic examples include:
- Brain zaps — brief electric-shock sensations in the head, often triggered by moving the eyes. These are close to pathognomonic for withdrawal; depression does not cause them. See our dedicated guide to brain zaps.
- Dizziness, vertigo, or feeling off-balance
- Nausea, stomach upset, flu-like aches
- Tingling, “electric” sensations, or heightened sensory sensitivity
Horowitz and Taylor put the logic plainly: if a surge of low mood and anxiety arrives alongside nausea, dizziness, and brain zaps, that combination points strongly to withdrawal rather than a mood relapse, because a depressive relapse does not typically come with electric-shock sensations. Relapse, by contrast, tends to look like the original episode — the same low mood, loss of interest, or anxiety you had before, without a new physical layer.
The catch is genuine overlap. Insomnia, anxiety, tearfulness, irritability, and poor concentration can belong to both withdrawal and relapse, and standard depression rating scales cannot separate them. That is exactly why the physical, novel symptoms carry so much diagnostic weight, and why the third clue — reinstatement — is so useful.
What happens when the dose is restored?
The third discriminator is the response to putting the dose back. Withdrawal symptoms typically resolve quickly once the previous stable dose is reinstated — often within days, and usually within about a week, per the pattern described by Horowitz and Taylor and by the Royal College of Psychiatrists. That rapid rescue is a strong signal that the problem was withdrawal, not relapse.
A genuine relapse does not behave that way. Restarting an antidepressant to treat a depressive episode usually takes weeks to show benefit, not days. So if restoring the dose settles things within a few days, withdrawal is the likely explanation; if there is little change after several days, relapse becomes more plausible.
Reinstatement is a recognized clinical strategy, not a personal experiment. The published approach is to return to the last dose at which you felt stable, allow time to settle, and then reduce again more gradually — a smaller step, over a longer interval. How to do that safely, and when to consider it, is covered in our hold-and-reinstate guide. Because it involves a dose change, it should be planned with your prescriber.
Did discontinuation trials confuse withdrawal with relapse?
This is where the personal question meets a bigger scientific debate. Most long-term “maintenance” recommendations rest on discontinuation trials: people who are well on an antidepressant are randomized either to keep taking it or to switch, often abruptly, to placebo. If the placebo group relapses more, the drug is credited with preventing relapse.
Critics argue this design is confounded. In these trials, switching to placebo is frequently done over just a few days — fast enough to provoke withdrawal. Michael Hengartner’s 2020 critical review (Therapeutic Advances in Psychopharmacology) notes that “relapses” cluster in the first few weeks after the switch, precisely when withdrawal risk peaks, and that the drug-placebo gap is largest early and then narrows. Typical figures are around a 40% “relapse” rate in the placebo arm versus about 20% in the continued-treatment arm at 12 months. Hengartner’s argument is that a substantial share of those early placebo-arm events are misclassified withdrawal, not true relapse — a follow-up analysis of trials submitted to the FDA (Hengartner & Plöderl, 2021) made the same case using time-to-event data. Horowitz and Taylor estimate that roughly 10 to 27 percentage points of the apparent relapses in these studies could be withdrawal in disguise.
Honest counterpoints, because the evidence is contested. This is not settled science, and the critique has serious critics of its own. Defenders of the maintenance trials point out that some studies did taper rather than stop abruptly and still found a drug-placebo difference, that not every early symptom return is withdrawal, and that untreated depression genuinely does recur. The high incidence and severity figures from Davies and Read (2019) drew methodological criticism for pooling heterogeneous studies and possible selection bias, and a 2025 reanalysis in Psychological Medicine argued that clinically meaningful withdrawal is less common than the highest estimates suggest. The fair summary: withdrawal confounding is real and was under-appreciated for years, but the exact size of its effect on relapse statistics is genuinely uncertain. Treat single headline percentages — in either direction — with caution, and label patient-community reports of very long or severe withdrawal as what they are: real lived experience that is not yet well quantified in controlled research.
Why does a dated symptom diary make this call so much easier?
Notice that all three discriminators are about pattern over time: how soon symptoms arrived after a dose change, whether new physical symptoms appeared, and how fast things settled after reinstatement. None of that can be reconstructed reliably from memory in a ten-minute appointment. Symptoms blur; the date of the last cut gets fuzzy; the brain zaps that dominated week one are forgotten by week three.
A dated diary that logs each dose, the date of every change, and daily symptoms turns a guessing game into a readable chart. When you can show your prescriber “the dizziness and zaps started three days after the cut, peaked at day ten, and eased within four days of going back up,” the withdrawal-versus-relapse question often answers itself. Horowitz and Taylor’s Maudsley Deprescribing Guidelines (2024) lean heavily on exactly this kind of temporal mapping.
This is the everyday problem RxDown is built for: a private day-by-day log of dose, symptoms, and sleep that produces a clear timeline and a shareable doctor report, plus a taper calculator for planning gradual, hyperbolic reductions. The diary is not a diagnostic tool — your prescriber makes the call — but it hands them the timing evidence they need to make it well.
What should I do in each case?
If the pattern looks like withdrawal — fast onset after a cut, novel physical symptoms, quick relief on reinstatement — the usual response is to stop reducing, return to the last comfortable dose, stabilize, and then taper more slowly with smaller steps. Understanding the windows and waves rhythm of recovery helps set realistic expectations. Bring your diary and use it to plan a gentler schedule with your prescriber; our guide on talking to your doctor about deprescribing has scripts for that conversation.
If the pattern looks like relapse — gradual onset unlinked to a dose change, symptoms that mirror your original episode, little response to reinstatement over several days — that is a signal to revisit the treatment plan itself rather than just the taper speed. That might mean restarting or continuing medication, adjusting it, or adding psychological support. This is a shared decision with your clinician, informed by your history and preferences.
When it is genuinely unclear, timing still helps: a brief, cautious trial of returning to the previous dose is often the fastest way to find out. Rapid improvement suggests withdrawal; a slow or absent response over a couple of weeks suggests relapse. That trial should be prescriber-led. The goal throughout is the same — reduce as slowly as your body needs, and never mistake the pain of stopping too fast for proof that you must keep taking the drug.
Sources
- Horowitz MA & Taylor D. Distinguishing relapse from antidepressant withdrawal: clinical practice and antidepressant discontinuation studies. BJPsych Advances (2022).
- Horowitz MA & Taylor D. Tapering of SSRI treatment to mitigate withdrawal symptoms. Lancet Psychiatry (2019).
- Davies J & Read J. A systematic review into the incidence, severity and duration of antidepressant withdrawal effects: Are guidelines evidence-based? Addictive Behaviors (2019).
- Hengartner MP. How effective are antidepressants for depression over the long term? A critical review of relapse prevention trials and the issue of withdrawal confounding. Therapeutic Advances in Psychopharmacology (2020).
- Hengartner MP & Plöderl M. Prophylactic effects or withdrawal reactions? An analysis of time-to-event data from antidepressant relapse prevention trials submitted to the FDA. Therapeutic Advances in Psychopharmacology (2021).
- Royal College of Psychiatrists. Stopping antidepressants (patient information resource).
- Horowitz MA & Taylor D. The Maudsley Deprescribing Guidelines: Antidepressants, Benzodiazepines, Gabapentinoids and Z-drugs. Wiley-Blackwell (2024).
Frequently asked questions
How soon do withdrawal symptoms start after reducing an antidepressant?
Withdrawal usually begins within a few days of a dose reduction and often peaks within a couple of weeks, according to the Royal College of Psychiatrists. Relapse of the original condition tends to build gradually over weeks to months. A long-half-life drug like fluoxetine can delay withdrawal onset by a week or two.
If my symptoms are withdrawal, will restoring the dose help quickly?
Usually, yes. Reinstating the last dose at which you felt stable typically eases withdrawal symptoms within days, often inside a week. A true relapse responds more slowly, on the timescale of weeks. Any dose change should be planned with your prescriber, not done on your own.
Can withdrawal really be mistaken for relapse?
Yes, and it happens often. Horowitz and Taylor argue that misclassified withdrawal inflated relapse rates in older discontinuation trials. Physical, novel symptoms such as brain zaps, dizziness, and nausea point toward withdrawal rather than a return of depression or anxiety.
Tracking your dose, sleep, and symptoms makes every conversation in this article easier. RxDown is a free diary built for exactly that. Get RxDown · Free taper calculator