Sleep and Medication Withdrawal: Why It Breaks, How to Protect It
⚕️ This article is education, not medical advice. Every claim is sourced below. Never stop or change medication without your prescriber — some medications are dangerous to stop abruptly.
TL;DR: Sleep is one of the first and most common casualties of a dose reduction because withdrawal pushes the nervous system into hyperarousal, and sleep is exquisitely sensitive to that state. When you reduce a sleep drug (a benzodiazepine or Z-drug) or a sedating antidepressant, the brain rebounds in the opposite direction — lighter sleep, vivid dreams, more awakenings. The single most evidence-based fix is not a new pill but cognitive behavioral therapy for insomnia (CBT-I), the first-line treatment endorsed by both the American College of Physicians and the American Academy of Sleep Medicine. Most withdrawal-related sleep disruption settles over days to weeks; when it doesn’t, that is a signal to slow the taper rather than push through.
This article is education, not medical advice. Any change to a psychiatric or sleep medication should be planned and supervised by your prescriber, and you should never stop these medications abruptly — abrupt discontinuation is the single biggest driver of severe withdrawal, including dangerous sleep and seizure risk with sedative-hypnotics.
Why is sleep usually the first thing to go when you cut a dose?
Two mechanisms stack up. The first is hyperarousal. Chronic insomnia researchers describe a well-supported “hyperarousal model” in which the sleeping brain shows elevated physiological, cognitive, and cortical activation — higher-frequency EEG activity and reduced GABA signaling that make it hard to switch off (Riemann et al., Sleep Medicine Reviews, 2010). Withdrawal is, in effect, a temporary hyperarousal state layered on top of whatever baseline you had. The nervous system has adapted to the drug’s calming presence, and when the dose drops, that adaptation is briefly unmasked as agitation, racing thoughts, and a body that won’t stand down at night.
The second mechanism is the mirror-image rule of drug withdrawal: symptoms tend to be the opposite of the drug’s original effects. A medication that made you sleepy and suppressed dreaming will, on reduction, tend to produce wakefulness and intense dreaming. This is why insomnia shows up so reliably. In antidepressant discontinuation, insomnia is prominent enough to earn a letter in the classic FINISH mnemonic — Flu-like symptoms, Insomnia, Nausea, Imbalance, Sensory disturbances, and Hyperarousal — first published to help clinicians remember the syndrome (Berber, Journal of Clinical Psychiatry, 1998). Notice that two of the six features, insomnia and hyperarousal, are directly about a nervous system that can’t settle.
Withdrawal itself is common and not always mild. A 2019 systematic review (Davies & Read, Addictive Behaviors, 97:111–121) found that roughly 56% of people who try to come off antidepressants experience withdrawal effects, and about 46% of those describe them as severe — a finding that challenged older guidance framing withdrawal as brief and trivial. Sleep is frequently part of that picture.
Rebound insomnia vs. withdrawal insomnia — what’s the difference?
These two terms get blurred, but they behave differently and matter for planning.
Rebound insomnia is a sharp, short-lived worsening of sleep below your pre-treatment baseline right after stopping or cutting a sleep-promoting drug. It is most associated with benzodiazepines and Z-drugs. The Ashton Manual explains the mechanism cleanly: benzodiazepines suppress both dreaming sleep (REM) and deep slow-wave sleep, so “on withdrawal, even after years of benzodiazepine use, there is a marked rebound increase in REMS which also becomes more intense,” making dreams vivid, sometimes producing nightmares and frequent awakenings (Ashton, Chapter 3). Rebound is worse with shorter-acting drugs. The Alliance for Sleep deprescribing guideline notes rebound is more severe with short-acting agents like triazolam, while for Z-drugs such as zolpidem and eszopiclone at standard doses it typically lasts only about one night (Watson et al., J Clin Med, 2023). If you are reducing these medications, see the benzodiazepine tapering guide (Ashton method) and the Z-drugs dependence reduction guide.
Withdrawal sleep disruption from antidepressants is different: a more prolonged, often waxing-and-waning disturbance rather than a single crash night. Reducing sedating antidepressants — mirtazapine (Remeron) or trazodone, both frequently prescribed off-label for sleep — removes a nightly source of sedation, so insomnia is both a discontinuation symptom and, sometimes, a rebound of the sleep problem the drug was masking. Because their sleep benefit was doing real work, the reduction can feel abrupt to your sleep system even when the mood dose is small.
| Feature | Rebound insomnia (benzos / Z-drugs) | Antidepressant withdrawal sleep disruption |
|---|---|---|
| Typical onset | Within 1–2 nights of a cut or stop | Within days of a dose change |
| Character | Sharp; sleep briefly worse than baseline | Fragmented sleep, vivid dreams, waxing/waning |
| Worst with | Short half-life agents (e.g., triazolam) | Sedating agents (mirtazapine, trazodone); short half-life (paroxetine, venlafaxine) |
| REM effect | Marked REM rebound, vivid dreams, nightmares | Vivid dreams reported, especially with sedating drugs |
| Usual course | Often resolves within days at standard doses | Days to several weeks; longer if taper is fast |
An important nuance: evidence on rebound is mixed. Some controlled studies of nightly zolpidem found little or no rebound on discontinuation, so rebound is a real pattern but not a certainty for everyone. The severity depends heavily on the drug, the dose, the duration of use, and how fast you come down.
Why does one bad night snowball into a bad week?
Poor sleep is not just another symptom on the list — it is an amplifier. Sleep loss lowers your threshold for anxiety, pain, irritability, and low mood, which are exactly the symptoms withdrawal is already producing. A rough night then feeds daytime worry about the next night, and that anticipatory arousal is precisely the cognitive hyperarousal that keeps chronic insomnia going (Riemann et al., 2010). Left unchecked, a few reduction-related bad nights can harden into a self-sustaining insomnia loop that outlasts the withdrawal itself.
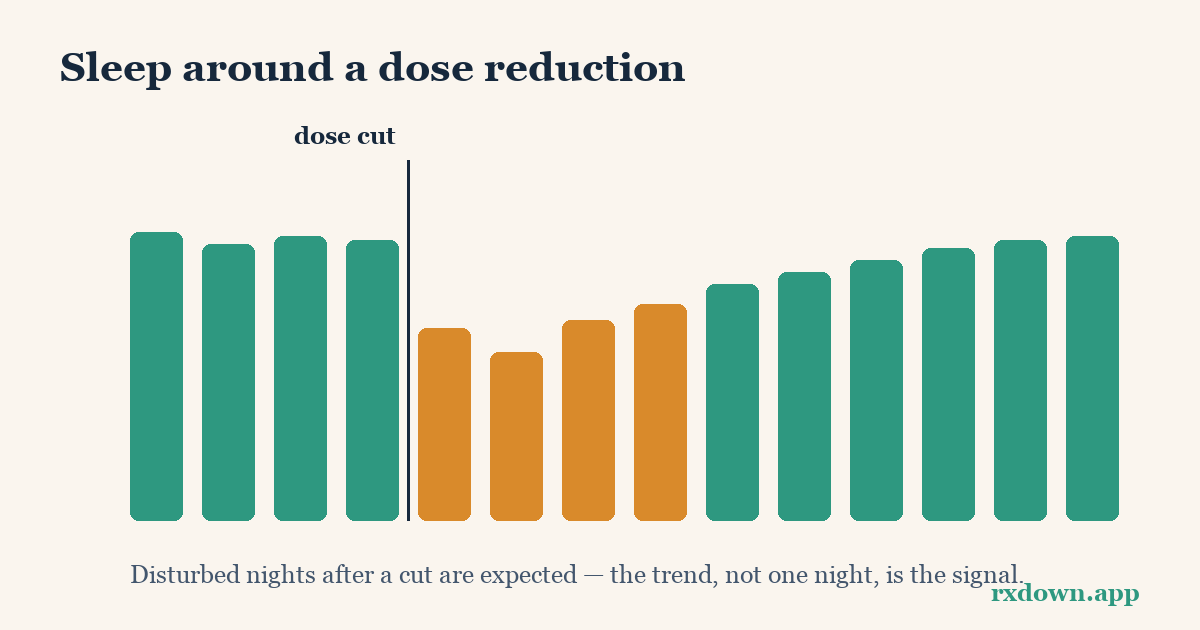
This is the strongest practical argument for tracking sleep during a taper. A single bad night is noise; a trend is signal. If you can see that your sleep dipped for three nights after a cut and then recovered, you can reassure yourself and hold your course. If instead the data show a steady multi-week decline, that is objective evidence to bring to your prescriber to slow down. Sleep data helps you tell a bad night from a bad trend — and that distinction is the difference between white-knuckling through unnecessary suffering and adjusting a plan that isn’t working. It also feeds directly into the harder question of discontinuation versus relapse.
What actually works: is CBT-I really better than a sleep pill?
For chronic insomnia, yes — the guideline evidence is unusually clear. In 2016 the American College of Physicians recommended that all adults receive CBT-I as the initial treatment for chronic insomnia disorder, reserving medication for shared-decision-making when CBT-I alone is insufficient, and noting drugs are FDA-approved mainly for short-term use of about four to five weeks (Qaseem et al., Annals of Internal Medicine, 2016). In 2021 the American Academy of Sleep Medicine went further, issuing a strong recommendation — its highest tier — that “clinicians use multicomponent cognitive behavioral therapy for insomnia for the treatment of chronic insomnia disorder in adults” (Edinger et al., J Clin Sleep Med, 2021).
CBT-I is not one technique but a small toolkit, usually delivered over four to eight sessions:
- Stimulus control — rebuilding the bed–sleep association: bed is for sleep only, get up if you can’t sleep, keep a fixed wake time. The AASM gives this a conditional recommendation as a stand-alone therapy.
- Sleep restriction — temporarily limiting time in bed to match actual sleep time, which consolidates fragmented sleep and increases sleep drive, then gradually expanding it. Also conditionally recommended stand-alone by the AASM.
- Cognitive work — addressing the catastrophic “I’ll never function tomorrow” thoughts that fuel nighttime arousal.
A 2024 component network meta-analysis of 241 trials (Furukawa et al., JAMA Psychiatry, 81:357–365) found that cognitive restructuring, sleep restriction, and stimulus control were the components most associated with benefit, while relaxation was potentially detrimental and — importantly — sleep hygiene appeared inert as a stand-alone intervention.
Crucially for tapering, CBT-I is not just a substitute for the drug you’re stopping; it can smooth the exit. The Alliance for Sleep guideline advises that when deprescribing, “BZDs should be tapered, preferably with some kind of behavioral therapy (e.g., CBT-I) or other support in place,” and one meta-analysis it cites found short-term CBT-I plus gradual tapering more effective for discontinuation than tapering alone (Watson et al., 2023).
Is sleep hygiene enough on its own?
Honestly, no — and it’s worth being clear about this so you don’t mistake a warm-up for the main event. Sleep hygiene (consistent schedule, dark cool room, limiting caffeine and alcohol, winding down off screens) is genuinely helpful and harms nothing. But both the AASM guideline and the 2024 component analysis found that sleep hygiene used alone is one of the weaker interventions: the AASM issued a conditional recommendation against using it as a single-component therapy for chronic insomnia. The practical takeaway is to treat sleep hygiene as the foundation you build CBT-I on top of, not as the treatment itself. During withdrawal specifically, a few basics carry extra weight: protect a fixed wake time, be cautious with alcohol (it worsens the REM rebound you’re already fighting), and avoid “catching up” with long daytime naps that steal your nighttime sleep drive.
What should I track, and why not just trust my memory?
Because memory is a poor instrument for sleep. People routinely misjudge how long they lay awake, and anxiety about sleep biases recall toward the worst nights — the same distortion that fuels the insomnia loop. Objective and semi-objective tracking corrects for this.
A practical minimum to log each day:
- Bedtime, wake time, and rough total sleep — to compute a trend, not to obsess over one figure.
- Number and length of awakenings — rebound tends to show up here first.
- A morning sleep-quality rating and daytime symptom rating — so you can line sleep up against mood, anxiety, and other withdrawal symptoms.
- Dose changes — the anchor everything else is compared against.
Wearables and phone platforms make the objective side easier: most consumer devices export sleep data to Apple Health or Android’s Health Connect, giving you nightly duration and stage estimates without a clinic. These are estimates, not lab polysomnography, but for spotting trends across a taper they are more reliable than recall. If you’re reducing a newer sleep drug, the mechanism-focused DORA sleep-medication discontinuation guide explains why some agents rebound less than others.
When do sleep problems mean I should slow down?
Some sleep disruption is an expected, self-limiting part of coming off these drugs. The question is when it crosses from “expected turbulence” to “the taper is too fast.” Signals that warrant a conversation about slowing, pausing, or holding include: insomnia that worsens rather than eases over two to three weeks after a cut; sleep loss severe enough to impair daytime safety or functioning; or new symptoms stacking on top (escalating anxiety, intrusive dreams, physical withdrawal signs).
The evidence-based response is usually to reduce more gradually, not to abandon the taper. The principle of hyperbolic tapering — proportionally smaller cuts as the dose gets lower, because receptor occupancy falls off steeply at the bottom — was formalized for antidepressants by Horowitz and Taylor (Lancet Psychiatry, 2019) and now underpins NICE guidance. Their protocol explicitly builds in the option to return to the previous dose if symptoms emerge, then proceed more slowly. That “hold and, if needed, step back” logic applies directly to sleep: if a cut wrecks your sleep, holding at the prior dose until sleep restabilizes is a legitimate, planned move, not a failure. See hold and reinstate, the hyperbolic tapering guide, and receptor occupancy explained for the mechanics, and remember that recovery often comes in windows and waves rather than a straight line. You can model gentler step sizes with the taper calculator.
How long until sleep recovers?
Timelines vary with the drug, dose, duration of use, and taper speed, so treat these as typical ranges rather than promises.
| Situation | Typical sleep-recovery pattern |
|---|---|
| Z-drug rebound (standard dose) | Often ~1 night to a few nights, per the Alliance for Sleep guideline |
| Short-acting benzodiazepine, gradual taper | Days to a few weeks per step; REM/dream rebound often eases as the deficit is repaid |
| Benzodiazepine REM rebound (Ashton) | Nightmares and vivid dreams “usually after about 4–6 weeks” become less frequent and fade |
| Antidepressant discontinuation insomnia | Often days to a few weeks; longer if the taper is fast or the drug was sedating |
| Slow, hyperbolic taper | Each small step disrupts sleep less, so recovery per step is usually shorter |
The Ashton Manual’s reassurance is worth holding onto: the drive to sleep is powerful, and “normal sleep will eventually reassert itself.” For antidepressants, remember that the older idea of withdrawal as reliably resolving in one to two weeks was overturned by the 2019 evidence — some people take longer, and a slower taper is the lever that most reliably shortens the ride. If sleep is your limiting symptom, that is useful information, not a verdict.
RxDown is built around exactly this kind of tracking. You can log dose changes, mood, and symptoms in the withdrawal diary, import objective sleep data from Apple Health or Health Connect so your sleep sits alongside every dose change, and generate a doctor report that turns those trends into something you can review with your prescriber — plus a taper calculator for planning gentler steps. The point isn’t more data for its own sake; it’s the ability to tell a bad night from a bad trend, and to make taper decisions from evidence instead of a single rough morning.
For more on individual drug classes and timelines, browse the sibling guides linked above or the FAQ. And whatever the data show, keep the reductions themselves in your prescriber’s hands.
Sources
- Qaseem A, et al., Management of Chronic Insomnia Disorder in Adults: ACP Clinical Practice Guideline, Annals of Internal Medicine (2016)
- Edinger JD, et al., Behavioral and Psychological Treatments for Chronic Insomnia Disorder in Adults: AASM Clinical Practice Guideline, Journal of Clinical Sleep Medicine (2021)
- Furukawa Y, et al., Components and Delivery Formats of CBT for Chronic Insomnia: A Component Network Meta-Analysis, JAMA Psychiatry (2024)
- Ashton CH, Benzodiazepines: How They Work and How to Withdraw (The Ashton Manual), Chapter 3 (2002)
- Watson NF, et al., Alliance for Sleep Clinical Practice Guideline on Switching or Deprescribing Hypnotic Medications for Insomnia, Journal of Clinical Medicine (2023)
- Horowitz MA, Taylor D, Tapering of SSRI treatment to mitigate withdrawal symptoms, Lancet Psychiatry (2019)
- Davies J, Read J, A systematic review into the incidence, severity and duration of antidepressant withdrawal effects, Addictive Behaviors (2019)
- Riemann D, et al., The hyperarousal model of insomnia: A review of the concept and its evidence, Sleep Medicine Reviews (2010)
- Berber MJ, FINISH: Remembering the discontinuation syndrome, Journal of Clinical Psychiatry (1998)
Frequently asked questions
Why does my sleep get worse when I lower my dose?
Withdrawal shifts the nervous system into a state of hyperarousal, and sleep is unusually sensitive to that shift. When you reduce a drug that suppressed dreaming or deep sleep — like a benzodiazepine, a Z-drug, or a sedating antidepressant — the brain rebounds in the opposite direction, causing lighter sleep, vivid dreams, and more awakenings. Insomnia is one of the most common early withdrawal symptoms across drug classes.
Is my insomnia a withdrawal effect or a sign my condition is coming back?
Timing and pattern are the clues. Withdrawal-driven insomnia usually appears within days of a dose change, often alongside other physical symptoms, and tends to ease over days to weeks. A returning underlying condition typically builds more gradually over weeks and comes with the mood or anxiety features that first led to treatment. Tracking sleep against your dose changes helps you and your prescriber tell the difference.
What is the most effective non-drug treatment for insomnia during a taper?
Cognitive behavioral therapy for insomnia (CBT-I) is the evidence-based first-line treatment for chronic insomnia, recommended by both the American College of Physicians (2016) and the American Academy of Sleep Medicine (2021). Its most active parts are stimulus control and sleep restriction, not sleep hygiene alone. CBT-I can be started in primary care or through validated digital programs.
Tracking your dose, sleep, and symptoms makes every conversation in this article easier. RxDown is a free diary built for exactly that. Get RxDown · Free taper calculator