Sleeping Pills vs. Sedatives: Are They the Same Thing?
⚕️ This article is education, not medical advice. Every claim is sourced below. Never stop or change medication without your prescriber — some medications are dangerous to stop abruptly.
TL;DR: “Sleeping pill,” “sedative,” “tranquilizer,” “hypnotic,” and “anxiolytic” are overlapping labels, not separate drug classes — and they often describe the very same medicine. Most prescription sleep and calming drugs sit under one pharmacological umbrella called sedative-hypnotics, whose effect grows with dose: light calming at low doses, sleep at higher ones. That is why a benzodiazepine can be a “tranquilizer” for daytime anxiety and a “sleeping pill” at night. But not every sleep aid is a classic sedative: melatonin-receptor agonists and dual orexin receptor antagonists (DORAs) work through different mechanisms and did not cause dependence or withdrawal in trials. The label on the box matters less than the drug class underneath — and that class is what decides how carefully you have to come off it. This article is education, not medical advice; never stop a sedative or sleep medication abruptly, and make any change with your prescriber.
Why do these words all seem to mean the same thing?
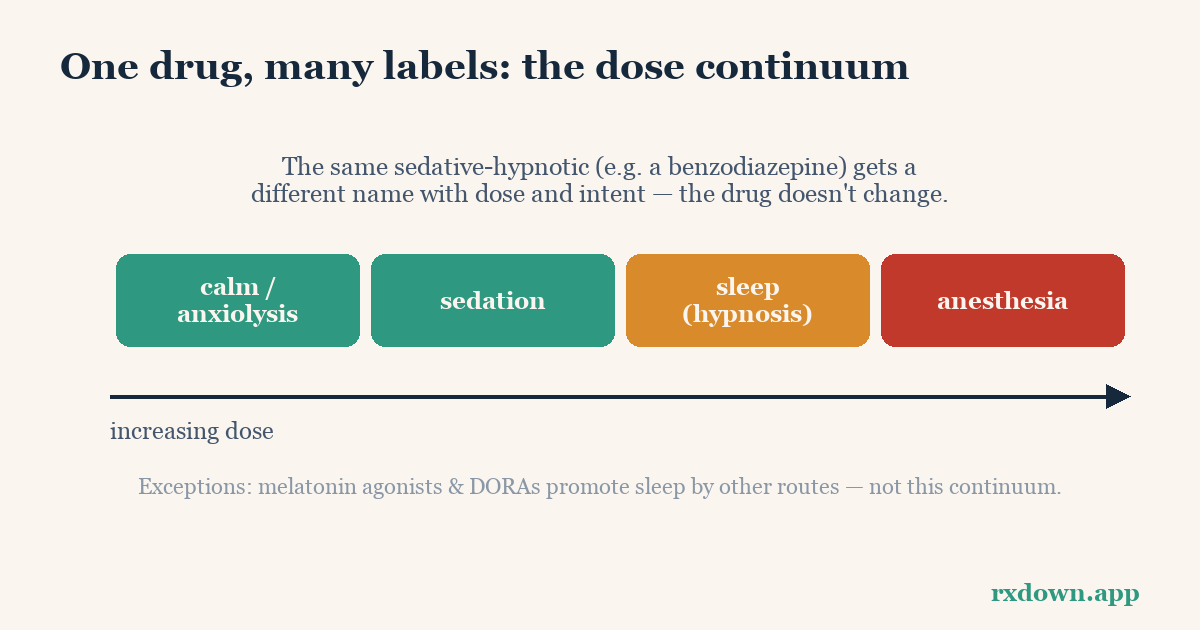
Because, chemically, many of them do. Pharmacology textbooks group the large majority of prescription calming and sleep drugs into a single family: sedative-hypnotics. As the StatPearls reference summarizes, these are drugs that “depress CNS function, inducing sedation, sleep, and unconsciousness with increasing dose.” In other words, the same drug can produce mild calm, then drowsiness, then full sleep, then anesthesia — depending only on how much is in your system.
That single fact explains most of the confusion:
- A sedative is a drug that calms and reduces excitement.
- A hypnotic is a drug that brings on or maintains sleep.
- An anxiolytic is a drug that reduces anxiety.
- A tranquilizer is an older, informal word for the same calming drugs — “minor tranquilizers” historically meant benzodiazepines used for anxiety, while “major tranquilizers” meant antipsychotics.
- A sleeping pill is a plain-language word for any of the above taken to help sleep.
These are descriptions of what a drug is being used for, layered on top of a dose continuum — not four different pharmacies of unrelated molecules. A low dose of a benzodiazepine sedates and relieves anxiety; a higher dose of the same benzodiazepine puts you to sleep. So the “anti-anxiety pill” and the “sleeping pill” in your cabinet may be chemically identical.
Is my “tranquilizer” the same as my “sleeping pill”?
Frequently, yes. The clearest example is the benzodiazepines. Diazepam (Valium), lorazepam (Ativan), and clonazepam (Klonopin) are usually called anti-anxiety drugs or “tranquilizers,” while temazepam (Restoril) and, in some countries, nitrazepam are marketed as sleeping pills. Pharmacologically they are the same class — positive modulators of the GABA-A receptor, the brain’s main “slow-down” system — differing mainly in how fast they act and how long they last, not in what they fundamentally do. The Ashton Manual, the standard reference on benzodiazepines, treats “sleeping” and “anxiety” benzodiazepines as one group precisely because they share mechanism, tolerance, and withdrawal behavior.
This is why you cannot judge a drug’s risk from the word on the label. “Sleeping pill” sounds gentler than “tranquilizer,” but if both are benzodiazepines, both carry the same potential for tolerance and dependence. If you’re not sure which class you’re taking, our companion guide on telling benzodiazepines, Z-drugs and DORAs apart walks through how to identify it.
Then are all sleep drugs sedatives? No — here’s the important exception
Not everything sold to help you sleep belongs to the sedative-hypnotic family. Two newer classes promote sleep without being broad CNS depressants, and that difference changes how they behave when you stop:
- Melatonin-receptor agonists (ramelteon/Rozerem, and melatonin itself). Ramelteon binds MT1 and MT2 melatonin receptors in the brain’s clock and, as its review literature notes, “has no appreciable affinity” for the GABA, dopamine, opioid, or serotonin receptors linked to classic sedation. It is the one prescription insomnia drug that is not a DEA-scheduled controlled substance, and it has not been associated with dependence or a withdrawal syndrome.
- Dual orexin receptor antagonists (DORAs) — daridorexant (Quviviq), lemborexant (Dayvigo), suvorexant (Belsomra). Rather than amplifying the brain’s brake (GABA), they block orexin, the brain’s wake signal. In their phase 3 trials and FDA labels, abrupt discontinuation did not produce rebound insomnia or measurable withdrawal — a genuine pharmacological break from the older hypnotics (see our DORA guide).
So “is my sleep drug a sedative?” has a real answer that depends on the molecule: benzodiazepines and Z-drugs, yes; DORAs and melatonin agonists, no.
A map of the labels
| Common label | What it usually means | Typical examples | GABA sedative-hypnotic? | Dependence / withdrawal risk |
|---|---|---|---|---|
| Benzodiazepine (“tranquilizer”) | Calms anxiety and/or induces sleep | diazepam, lorazepam, clonazepam, temazepam | Yes | Meaningful — usually needs a taper |
| Z-drug (“sleeping pill”) | Non-benzodiazepine hypnotic for sleep | zolpidem, zopiclone, eszopiclone | Yes (same GABA site) | Meaningful — usually needs a taper |
| DORA | Blocks the wake signal (orexin) | daridorexant, lemborexant, suvorexant | No | Low; no withdrawal seen in trials |
| Melatonin agonist | Acts on the body clock | ramelteon, melatonin | No | Low; not a controlled substance |
| Sedating antidepressant (off-label for sleep) | Antidepressant used at low dose for sleep | trazodone, mirtazapine, low-dose doxepin | No | Can cause discontinuation effects (antidepressant class) |
| Sedating antihistamine (OTC “sleep aid”) | Older allergy drugs that cause drowsiness | diphenhydramine, doxylamine | No | Tolerance to the sleep effect is common |
The table also shows why over-the-counter “sleep aids” (usually antihistamines) and low-dose antidepressants used for sleep sit outside the sedative-hypnotic family — they are different drugs pressed into the sleep role, each with their own considerations.
Why the label matters most when you want to stop
Here is the practical payoff. The risk of a physical withdrawal syndrome does not track the word on the box — it tracks the drug class:
- Benzodiazepines and Z-drugs act on GABA, and the nervous system adapts to their presence. Stop suddenly and that adaptation is unmasked, which can mean rebound insomnia, surging anxiety, and — with benzodiazepines especially — genuinely dangerous effects including seizures. These usually require a slow, individualized taper. NICE lists both among “medicines associated with dependence or withdrawal symptoms.”
- DORAs and melatonin agonists did not show a withdrawal syndrome in their studies, so the main issue on stopping is whether your original sleep problem returns — a treatment question, not a withdrawal one.
That is the reason the pharmacology, not the marketing, should guide your plan. Someone stopping a “sleeping pill” that turns out to be a benzodiazepine needs a very different, much more cautious approach than someone stopping a DORA. If your underlying problem is chronic insomnia, guidelines from the American College of Physicians recommend cognitive behavioral therapy for insomnia (CBT-I) as the first-line, durable treatment — so coming off a hypnotic is often paired with starting CBT-I rather than simply removing the drug.
The bottom line
“Sleeping pill,” “sedative,” “tranquilizer,” “hypnotic,” and “anxiolytic” are overlapping everyday and clinical labels, and for the GABA drugs they frequently name the very same medicine at different doses or times of day. What actually determines how a drug behaves — and how carefully you must come off it — is its pharmacological class: benzodiazepines and Z-drugs are dependence-forming sedative-hypnotics that usually need a taper, while DORAs and melatonin agonists work differently and were not linked to withdrawal. Identify the class, not the label, and plan any change with your prescriber. To learn which class you’re on, read Know your medication: BZD vs Z-drug vs DORA; when you’re ready to think about stopping, see when and how to start tapering or the taper calculator. More common questions are answered in the FAQ.
Sources
- Anxiolytics and Sedative-Hypnotics Toxicity, StatPearls, NCBI Bookshelf (2023)
- Ashton CH, Benzodiazepines: How They Work and How to Withdraw (The Ashton Manual, 2002/rev. 2011)
- Qaseem A et al., Management of Chronic Insomnia Disorder in Adults, Annals of Internal Medicine (2016)
- U.S. FDA, Boxed Warning for Certain Prescription Insomnia Medicines (2019)
- Mignot E, et al., Safety and efficacy of daridorexant in adults with insomnia disorder, Lancet Neurology (2022)
- Simpson D, Curran MP, Ramelteon: A Review of its Use in Insomnia, Drugs / PMC (2008)
- NICE, Medicines associated with dependence or withdrawal symptoms (NG215) (2022)
Frequently asked questions
Are sleeping pills and sedatives the same thing?
Often, yes — many are the same drugs used at different doses or times of day. Pharmacologists group most of them under one umbrella, 'sedative-hypnotics.' A benzodiazepine like diazepam can be called a 'sedative' or 'tranquilizer' when used for anxiety and a 'sleeping pill' when taken at night; the drug is identical, only the label and intent change. Not every sleep aid is a classic sedative, though: melatonin-receptor agonists and dual orexin receptor antagonists (DORAs) promote sleep through different mechanisms and are not sedative-hypnotics in the dependence-forming sense.
What is the difference between a hypnotic and an anxiolytic?
A hypnotic is meant to bring on or maintain sleep; an anxiolytic (anti-anxiety drug) is meant to reduce anxiety. The distinction is mostly about dose and intended use rather than the drug itself: many sedatives calm anxiety at lower doses and induce sleep at higher ones, which is why the same medicine can wear both labels. The older term 'minor tranquilizer' referred mainly to benzodiazepines used for anxiety.
Does it matter which type I'm taking when I want to stop?
Yes, a great deal. The GABA-based sedative-hypnotics — benzodiazepines and Z-drugs — can cause tolerance, physical dependence, and a withdrawal syndrome, so they usually need a slow, planned taper. DORAs and melatonin agonists were not associated with withdrawal or rebound in their trials. Knowing your drug's class tells you whether abrupt stopping is merely uncomfortable or genuinely risky, so always confirm with your prescriber before changing anything.
Tracking your dose, sleep, and symptoms makes every conversation in this article easier. RxDown is a free diary built for exactly that. Get RxDown · Free taper calculator